

MICE models: superior to the HERG model in predicting Torsade de Pointes
- PMID: 23812503
- PMCID: PMC3696896
- DOI: 10.1038/srep02100
MICE models: superior to the HERG model in predicting Torsade de Pointes
Abstract
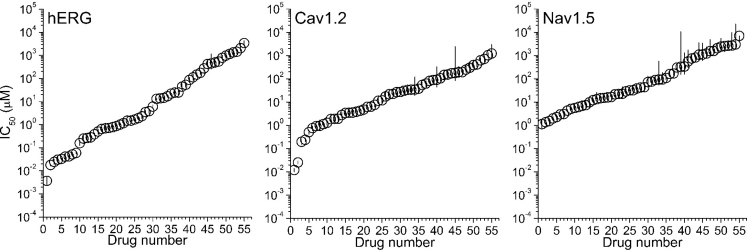
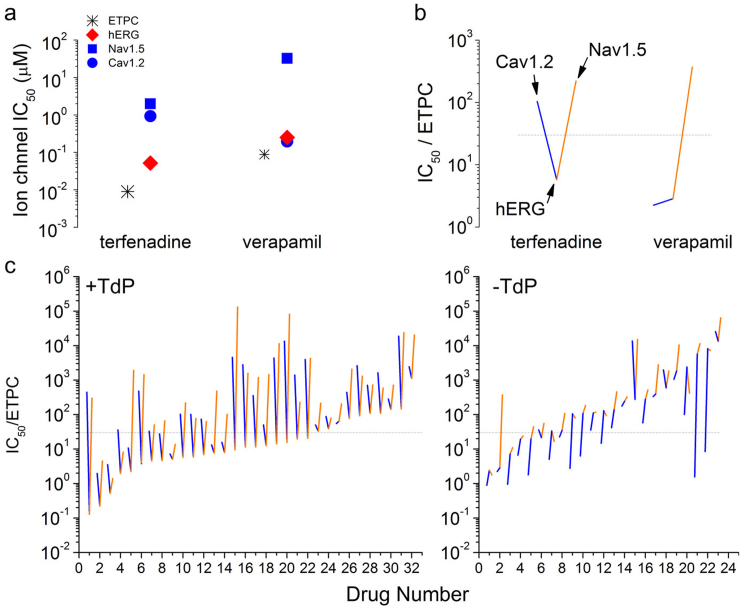
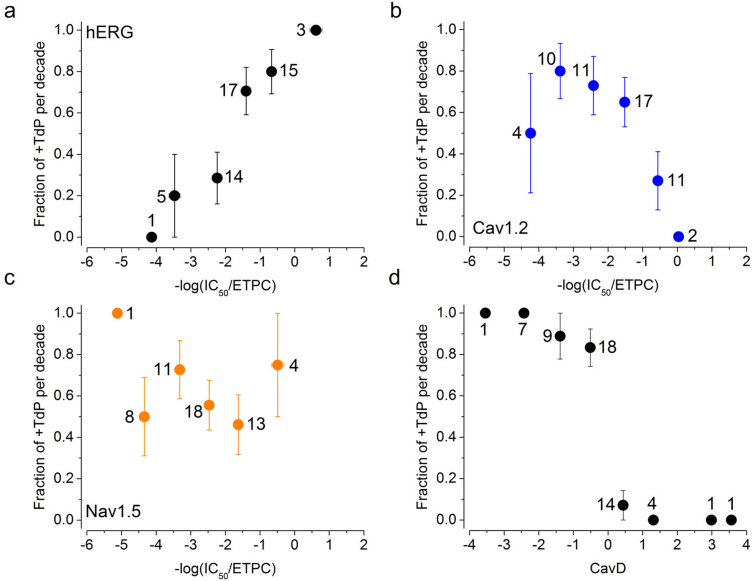
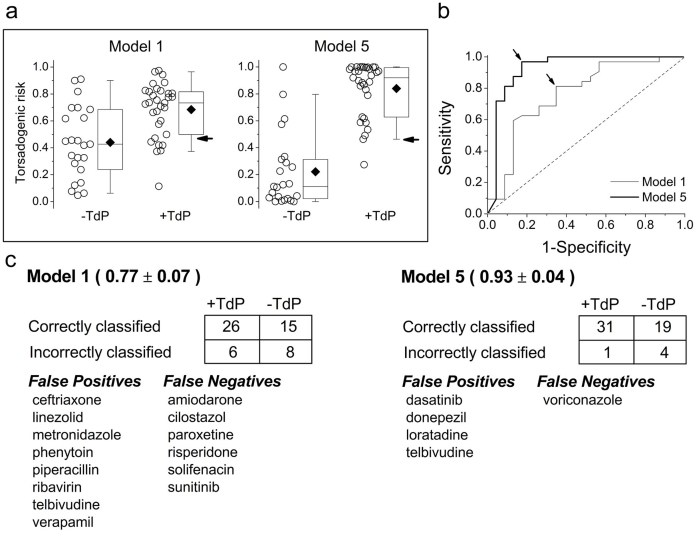
Drug-induced block of the cardiac hERG (human Ether-à-go-go-Related Gene) potassium channel delays cardiac repolarization and increases the risk of Torsade de Pointes (TdP), a potentially lethal arrhythmia. A positive hERG assay has been embraced by regulators as a non-clinical predictor of TdP despite a discordance of about 30%. To test whether assaying concomitant block of multiple ion channels (Multiple Ion Channel Effects or MICE) improves predictivity we measured the concentration-responses of hERG, Nav1.5 and Cav1.2 currents for 32 torsadogenic and 23 non-torsadogenic drugs from multiple classes. We used automated gigaseal patch clamp instruments to provide higher throughput along with accuracy and reproducibility. Logistic regression models using the MICE assay showed a significant reduction in false positives (Type 1 errors) and false negatives (Type 2 errors) when compared to the hERG assay. The best MICE model only required a comparison of the blocking potencies between hERG and Cav1.2.
Figures
References
-
- S7B Nonclinical Evaluation of the Potential for Delayed Ventricular Repolarization (QT Interval Prolongation) by Human Pharmaceuticals (October2005). - PubMed
-
- Sanguinetti M. C., Jiang C., Curran M. E. & Keating M. T. A mechanistic link between an inherited and an acquired cardiac arrhythmia: HERG encodes the IKr potassium channel. Cell. 81, 299–307 (1995). - PubMed
-
- Roy M., Dumaine R. & Brown A. M. HERG, a primary human ventricular target of the nonsedating antihistamine terfenadine. Circulation. 94, 817–823 (1996). - PubMed
-
- Suessbrich H., Waldegger S., Lang F. & Busch A. E. Blockade of HERG channels expressed in Xenopus oocytes by the histamine receptor antagonists terfenadine and astemizole. FEBS Lett. 385, 77–80 (1996). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Chemical Information
