

A systematic review with meta-analysis of posterior interbody fusion versus posterolateral fusion in lumbar spondylolisthesis
- PMID: 23812825
- PMCID: PMC3897839
- DOI: 10.1007/s00586-013-2880-8
A systematic review with meta-analysis of posterior interbody fusion versus posterolateral fusion in lumbar spondylolisthesis
Abstract
Purpose: To compare the clinical effectiveness of posterior lumbar interbody fusion (PLIF) and posterolateral fusion (PLF) for lumbar spondylolisthesis and to collect scientific evidence for determining which fusion method is better.
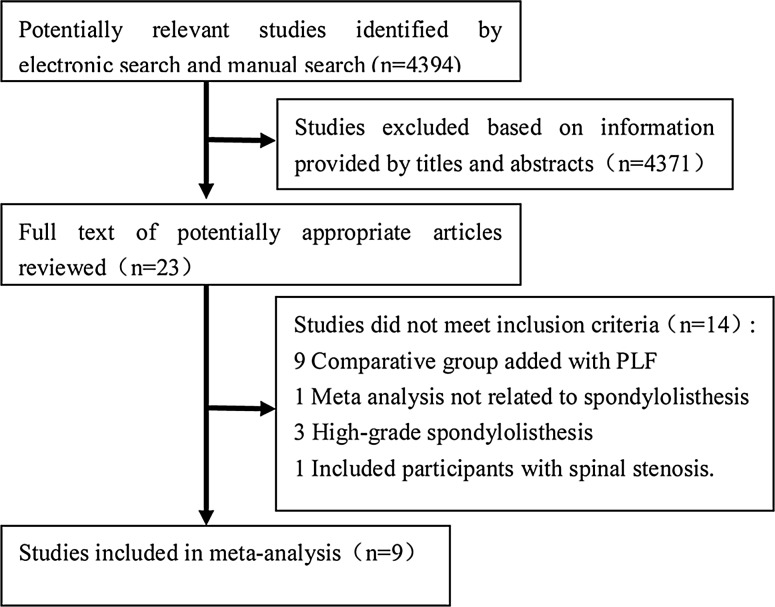
Methods: After systematic search, comparative studies were selected according to eligibility criteria. Checklists by Furlan and by Cowley were used to evaluate the risk of bias of the included randomized controlled trials (RCTs) and nonrandomized controlled studies, respectively. Weighed mean differences (WMDs) and risk differences were calculated for common outcomes. The final strength of evidence was expressed as different levels recommended by the GRADE Working Group.
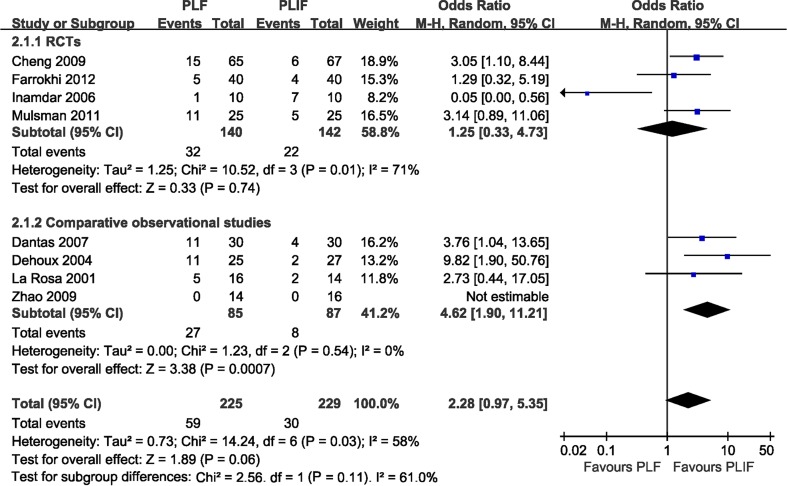
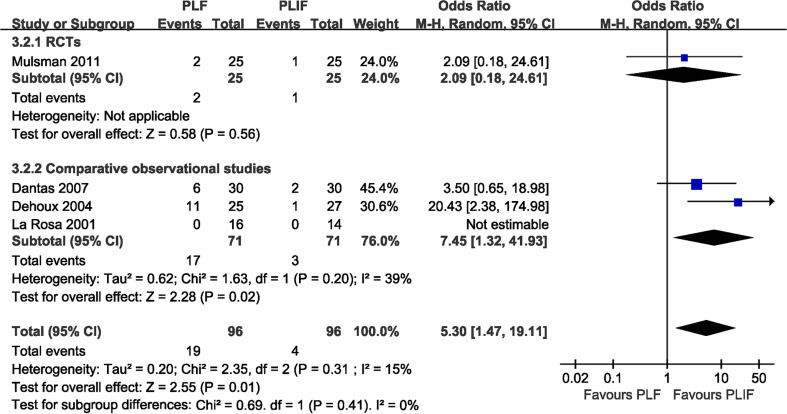
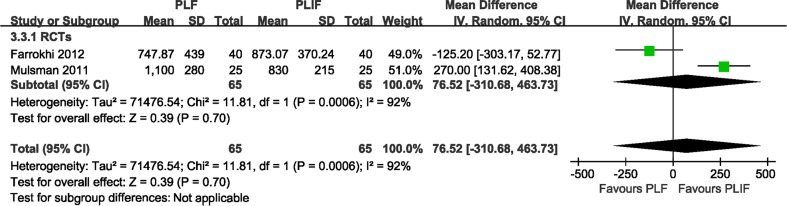
Results: Four RCTs and five comparative observational studies were identified. Moderate-quality evidence indicated that PLIF was more effective than PLF for clinical satisfaction [odds ratios (OR) 0.49, 95 % confidence limits (95 % CI): (0.28, 0.88, P = 0.02)]. Moderate-quality evidence showed that no significant difference was found for the complication rate [OR 2.28, 95 % CI (0.97, 5.35), P = 0.06]. In secondary outcomes, moderate-quality evidence indicated that PLIF improved fusion rate [OR 0.32, 95 % CI (0.17, 0.61), P = 0.0006]. Low-quality evidence showed that PLIF resulted in a lower reoperation rate than PLF [OR 5.30, 95 % CI (1.47, 19.11), P = 0.01]. No statistical difference was found between the two groups with regard to blood loss [WMD = 76.52, 95 % CI (-310.68, 463.73), P = 0.70] and operating time [WMD = -1.20, 95 % CI (-40.36, 37.97), P = 0.95].
Conclusions: Moderate-quality evidence indicates that PLIF can improve the clinical satisfaction and increase the fusion rate compared to PLF. No superiority was found between the two fusion methods in terms of complication rate, amount of blood loss, and operating time for the treatment of lumbar spondylolisthesis.
Figures




Comment in
-
Letter regarding Liu et al.'s study entitled "A systematic review with meta-analysis of posterior interbody fusion versus posterolateral fusion in lumbar spondylolisthesis".Eur Spine J. 2014 Apr;23(4):933-4. doi: 10.1007/s00586-014-3167-4. Epub 2014 Jan 17. Eur Spine J. 2014. PMID: 24435984 Free PMC article. No abstract available.
-
Answer to the Letter to the Editor of Feng Li et al. entitled "A systematic review with meta-analysis of posterior interbody fusion versus posterolateral fusion in lumbar spondylolisthesis" by Xiaoyang Liu, Yipeng Wang, Guixing Qiu, Xisheng Weng, Bin Yu. Eur Spine J (2013): doi:10.1007/s00586-013-2880-8.Eur Spine J. 2014 Apr;23(4):935-7. doi: 10.1007/s00586-014-3172-7. Epub 2014 Jan 22. Eur Spine J. 2014. PMID: 24448895 Free PMC article. No abstract available.
References
-
- Kim NH, Lee JW (1999) Anterior interbody fusion versus posterolateral fusion with transpedicular fixation for isthmic spondylolisthesis in adults. A comparison of clinical results. Spine (Phila Pa 1976) 24:812–816, 817 - PubMed
-
- Lin PM. Posterior lumbar interbody fusion technique: complications and pitfalls. Clin Orthop Relat Res. 1985;193:90–102. - PubMed
-
- DeWald RL, Faut MM, Taddonio RF, Neuwirth MG. Severe lumbosacral spondylolisthesis in adolescents and children. Reduction and staged circumferential fusion. J Bone Joint Surg Am. 1981;63:619–626. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
