

Seven-tesla phase imaging of acute multiple sclerosis lesions: a new window into the inflammatory process
- PMID: 23813441
- PMCID: PMC3812397
- DOI: 10.1002/ana.23959
Seven-tesla phase imaging of acute multiple sclerosis lesions: a new window into the inflammatory process
Abstract
Objective: In multiple sclerosis (MS), accurate, in vivo characterization of dynamic inflammatory pathological changes occurring in newly forming lesions could have major implications for understanding disease pathogenesis and mechanisms of tissue destruction. Here, we investigated the potential of ultrahigh-field magnetic resonance imaging (MRI; 7T), particularly phase imaging combined with dynamic contrast enhancement, to provide new insights in acute MS lesions.
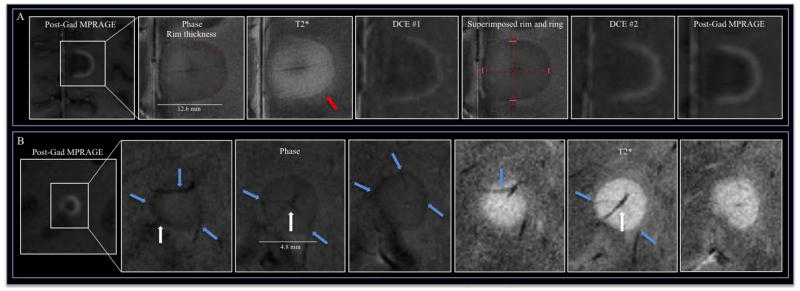
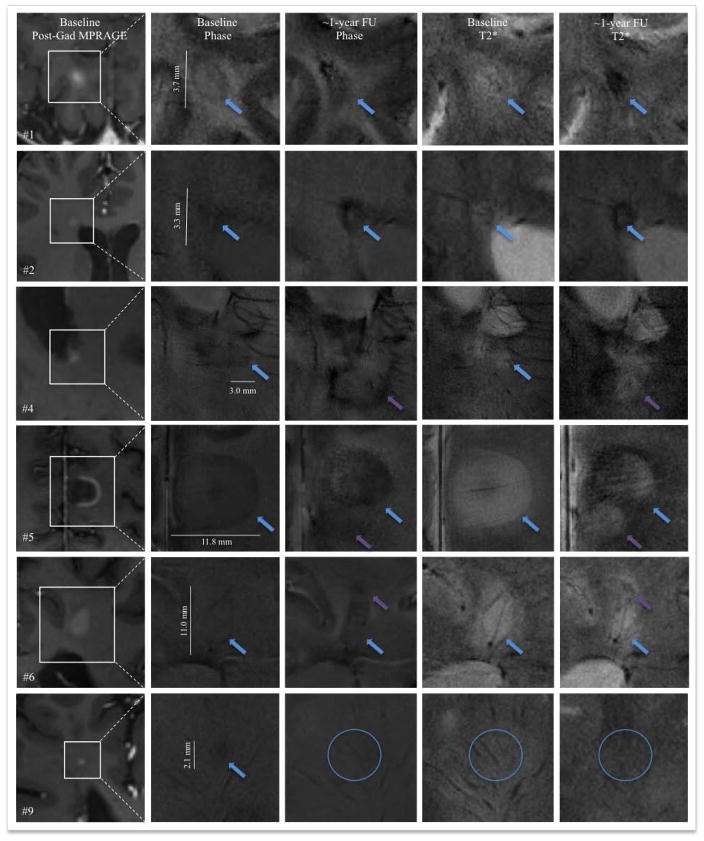
Methods: Sixteen active MS patients were studied at 7T. Noncontrast, high-resolution T2* magnitude and phase scans, T1 scans before/after gadolinium contrast injection, and dynamic contrast-enhanced (DCE) T1 scans were acquired. T2*/phase features and DCE pattern were determined for acute and chronic lesions. When possible, 1-year follow-up 7T MRI was performed.
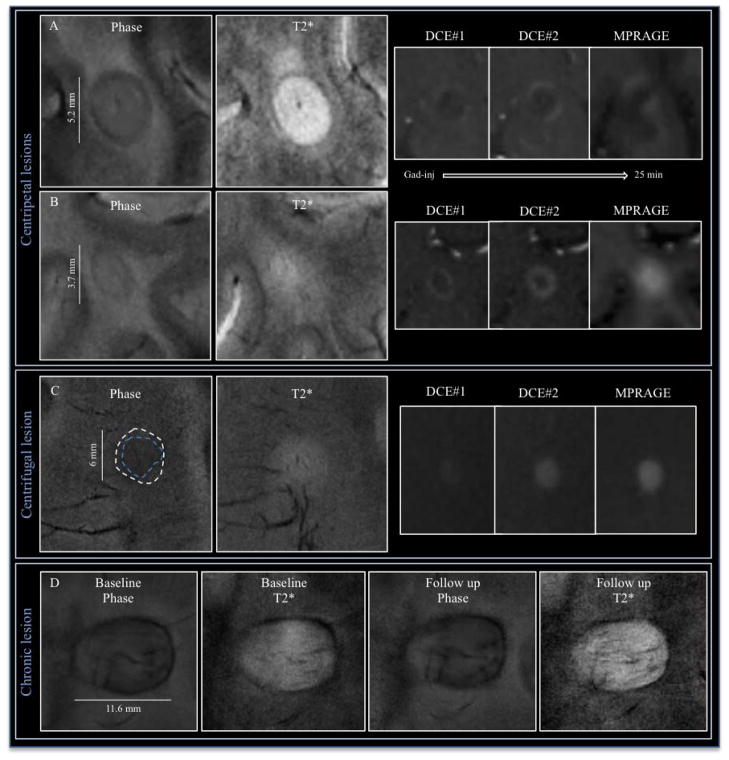
Results: Of 49 contrast-enhancing lesions, 44 could be analyzed. Centrifugal DCE lesions appeared isointense or hypointense on phase images, whereas centripetal DCE lesions showed thin, hypointense phase rims that clearly colocalized with the initial site of contrast enhancement. This pattern generally disappeared once enhancement resolved. Conversely, in 43 chronic lesions also selected for the presence of hypointense phase rims, the findings were stable over time, and the rims were typically thicker and darker. These considerations suggest different underlying pathological processes in the 2 lesion types.
Interpretation: Ultrahigh-field MRI and, especially, phase contrast, are highly sensitive to tissue changes in acute MS lesions, which differ from the patterns seen in chronic lesions. In acute lesions, the hypointense phase rim reflects the expanding inflammatory edge and may directly correspond to inflammatory byproducts and sequelae of blood-brain barrier opening.
© 2013 American Neurological Association.
Figures
References
-
- Barnett MH, Prineas JW. Relapsing and remitting multiple sclerosis: pathology of the newly forming lesion. Ann Neurol. 2004;55:458–468. - PubMed
-
- Henderson AP, Barnett MH, Parratt JD, Prineas JW. Multiple sclerosis: distribution of inflammatory cells in newly forming lesions. Ann Neurol. 2009;66:739–753. - PubMed
-
- Hu W, Lucchinetti CF. The pathological spectrum of CNS inflammatory demyelinating diseases. Seminars in immunopathology. 2009;31:439–453. - PubMed
-
- Prineas JW, Parratt JD. Oligodendrocytes and the early multiple sclerosis lesion. Ann Neurol. 2012;72:18–31. - PubMed
-
- Popescu BF, Lucchinetti CF. Pathology of demyelinating diseases. Annual review of pathology. 2012;7:185–217. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
