

Glomerular diseases: membranous nephropathy--a modern view
- PMID: 23813556
- PMCID: PMC3944756
- DOI: 10.2215/CJN.04160413
Glomerular diseases: membranous nephropathy--a modern view
Abstract
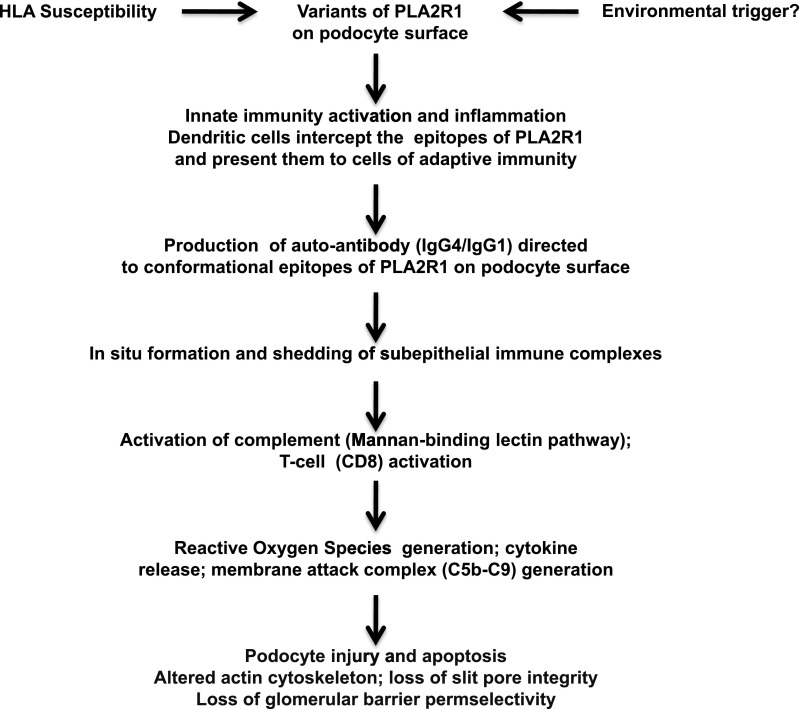
Membranous nephropathy (MN) is an autoimmune disease usually associated with a nephrotic syndrome and it may progress to ESRD in the long term. Its etiology is often unknown (idiopathic MN), whereas other cases have a recognizable etiology (secondary MN). In idiopathic MN, the glomerular lesions are mainly caused by autoantibodies against a podocyte membrane protein, the M-type of phospholipase A2 receptor 1. The natural course of idiopathic MN is quite varied with spontaneous complete or partial remissions a relatively common occurrence. Patients with asymptomatic non-nephrotic proteinuria seldom progress and need only conservative management. Those with persistent full-blown nephrotic syndrome and those with declining renal function are candidates for specific treatment with any of several regimens. Cyclical therapy with alternating monthly intravenous and oral glucocorticoids combined with a cytotoxic agent can induce remission and preserve renal function in the long term. Cyclosporine or tacrolimus can induce remission, but relapses are frequent after the drug withdrawal. Mycophenolate mofetil monotherapy seems to be ineffective, but may be beneficial when administered together with steroids. The experience with adrenocorticotropic hormone, natural or synthetic, is limited to a few studies with short-term follow-up, but high rates of remission can be seen after prolonged treatment. A high rate of remission and good tolerance have also been reported with rituximab. Patients with moderate renal insufficiency may also benefit from treatment, but at a price of frequent and serious side effects. With these limitations in mind, idiopathic MN may be considered a treatable disease in many patients.
Figures
References
-
- Stanescu HC, Arcos-Burgos M, Medlar A, Bockenhauer D, Kottgen A, Dragomirescu L, Voinescu C, Patel N, Pearce K, Hubank M, Stephens HA, Laundy V, Padmanabhan S, Zawadzka A, Hofstra JM, Coenen MJ, den Heijer M, Kiemeney LA, Bacq-Daian D, Stengel B, Powis SH, Brenchley P, Feehally J, Rees AJ, Debiec H, Wetzels JF, Ronco P, Mathieson PW, Kleta R: Risk HLA-DQA1 and PLA(2)R1 alleles in idiopathic membranous nephropathy. N Engl J Med 364: 616–626, 2011 - PubMed
-
- Coenen MJ, Hofstra JM, Debiec H, Stanescu HC, Medlar AJ, Stengel B, Boland-Augé A, Groothuismink JM, Bockenhauer D, Powis SH, Mathieson PW, Brenchley PE, Kleta R, Wetzels JF, Ronco P: Phospholipase A2 receptor (PLA2R1) sequence variants in idiopathic membranous nephropathy. J Am Soc Nephrol 24: 677–683, 2013 - PMC - PubMed
-
- Salant DJ: Genetic variants in membranous nephropathy: Perhaps a perfect storm rather than a straightforward conformeropathy? J Am Soc Nephrol 24: 525–528, 2013 - PubMed
-
- Murtas C, Bruschi M, Candiano G, Moroni G, Magistroni R, Magnano A, Bruno F, Radice A, Furci L, Argentiero L, Carnevali ML, Messa P, Scolari F, Sinico RA, Gesualdo L, Fervenza FC, Allegri L, Ravani P, Ghiggeri GM: Coexistence of different circulating anti-podocyte antibodies in membranous nephropathy. Clin J Am Soc Nephrol 7: 1394–1400, 2012 - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
