

Adverse outcomes among women presenting with signs and symptoms of ischemia and no obstructive coronary artery disease: findings from the National Heart, Lung, and Blood Institute-sponsored Women's Ischemia Syndrome Evaluation (WISE) angiographic core laboratory
- PMID: 23816032
- PMCID: PMC3703586
- DOI: 10.1016/j.ahj.2013.04.002
Adverse outcomes among women presenting with signs and symptoms of ischemia and no obstructive coronary artery disease: findings from the National Heart, Lung, and Blood Institute-sponsored Women's Ischemia Syndrome Evaluation (WISE) angiographic core laboratory
Abstract
Background: Women presenting with signs and symptoms of myocardial ischemia frequently have no or nonobstructive coronary artery disease (CAD).
Objective: This study aimed to investigate the associations between angiographic measures and longer-term clinical outcomes among women with signs and symptoms of ischemia referred for coronary angiography.
Methods: A prospective cohort analysis of women referred for coronary angiography and enrolled in the National Heart, Lung, and Blood Institute-sponsored WISE was performed. An angiographic severity score was prospectively developed, assigning points for any stenosis weighted by stenosis severity, location, and collaterals and was then tested for prediction for adverse outcome in 917 women, over a median of 9.3 years.
Setting: The study was conducted in referral centers.
Patients: Women with signs and/or symptoms of myocardial ischemia referred for coronary angiography were consecutively consented and enrolled in a prospective study.
Main outcome measures: Main outcomes included first occurrence of cardiovascular death or nonfatal myocardial infarction. Hospitalization for angina was a secondary outcome.
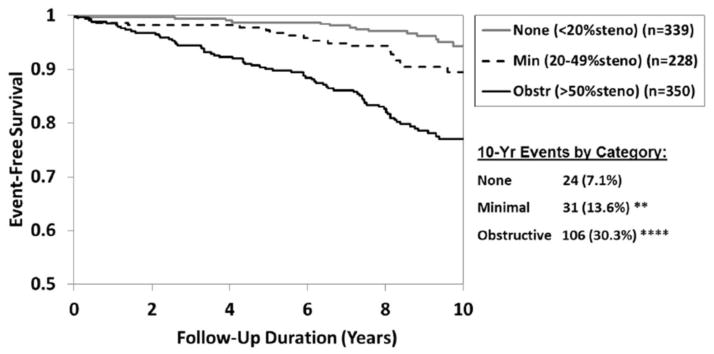
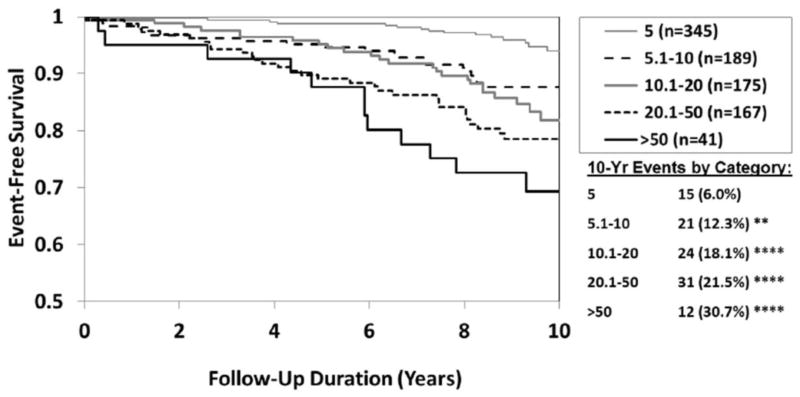
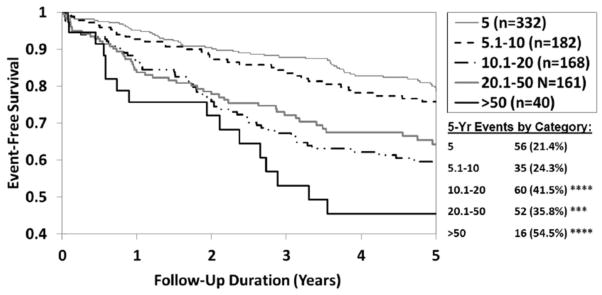
Results: Cardiovascular death or myocardial infarction at 10 years occurred in 6.7%, 12.8%, and 25.9% of women with no, nonobstructive, and obstructive CAD (P < .0001), respectively. Cumulative 10-year cardiovascular death or myocardial infarction rates showed progressive, near-linear increases for each WISE CAD severity score range of 5, 5.1 to 10, 10.1 to 20, 20.1 to 50, and >50. The optimal threshold in the WISE severity score classifications for predicting cardiovascular mortality was >10 (eg, 5.0-10 vs 10.1-89), with both a sensitivity and specificity of 0.64 and an area under the curve of 0.64 (P = .02, 95% CI 0.59-0.68).
Conclusions: Among women with signs and symptoms of ischemia, nonobstructive CAD is common and associated with adverse outcomes over the longer term. The new WISE angiographic score appears to be useful for risk prediction in this population.
Trial registration: ClinicalTrials.gov NCT00000554.
Copyright © 2013 Mosby, Inc. All rights reserved.
Conflict of interest statement
Figures
References
-
- Shaw LJ, Merz CN, Pepine CJ, Reis SE, Bittner V, Kip KE, et al. The economic burden of angina in women with suspected ischemic heart disease: results from the National Institutes of Health--National Heart, Lung, and Blood Institute--sponsored Women’s Ischemia Syndrome Evaluation. Circulation. 2006;114(9):894–904. - PubMed
-
- O’Donoghue M, Boden WE, Braunwald E, Cannon CP, Clayton TC, de Winter RJ, et al. Early invasive vs conservative treatment strategies in women and men with unstable angina and non-ST-segment elevation myocardial infarction: a meta-analysis. Jama. 2008;300(1):71–80. - PubMed
-
- Jespersen L, Hvelplund A, Abildstrom SZ, Pedersen F, Galatius S, Madsen JK, et al. Stable angina pectoris with no obstructive coronary artery disease is associated with increased risks of major adverse cardiovascular events. Eur Heart J. 2012;33(6):734–44. - PubMed
-
- Glaser R, Herrmann HC, Murphy SA, Demopoulos LA, DiBattiste PM, Cannon CP, et al. Benefit of an early invasive management strategy in women with acute coronary syndromes. Jama. 2002;288(24):3124–9. - PubMed
-
- Faxon DP, McCabe CH, Kreigel DE, Ryan TJ. Therapeutic and economic value of a normal coronary angiogram. Am J Med. 1982;73(4):500–5. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
- N01 HV068161/HV/NHLBI NIH HHS/United States
- U0164829/PHS HHS/United States
- N01 HV068163/HL/NHLBI NIH HHS/United States
- R03 AG032631/AG/NIA NIH HHS/United States
- 1R03AG032631/AG/NIA NIH HHS/United States
- U01 HL649141/HL/NHLBI NIH HHS/United States
- U01 HL649241/HL/NHLBI NIH HHS/United States
- M01 RR000425/RR/NCRR NIH HHS/United States
- N01-HV-68163/HV/NHLBI NIH HHS/United States
- MO1-RR00425/RR/NCRR NIH HHS/United States
- N01 HV068162/HL/NHLBI NIH HHS/United States
- R01-HL090957/HL/NHLBI NIH HHS/United States
- R01 HL090957/HL/NHLBI NIH HHS/United States
- T32 HL069751/HL/NHLBI NIH HHS/United States
- T32HL69751/HL/NHLBI NIH HHS/United States
- N01-HV-68162/HV/NHLBI NIH HHS/United States
- N01 HV068164/HV/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
