

Cutaneous and post kala-azar dermal leishmaniasis caused by Leishmania infantum in endemic areas of visceral leishmaniasis, northwestern Iran 2002-2011: a case series
- PMID: 23816511
- PMCID: PMC4001470
- DOI: 10.1179/2047773213Y.0000000097
Cutaneous and post kala-azar dermal leishmaniasis caused by Leishmania infantum in endemic areas of visceral leishmaniasis, northwestern Iran 2002-2011: a case series
Abstract
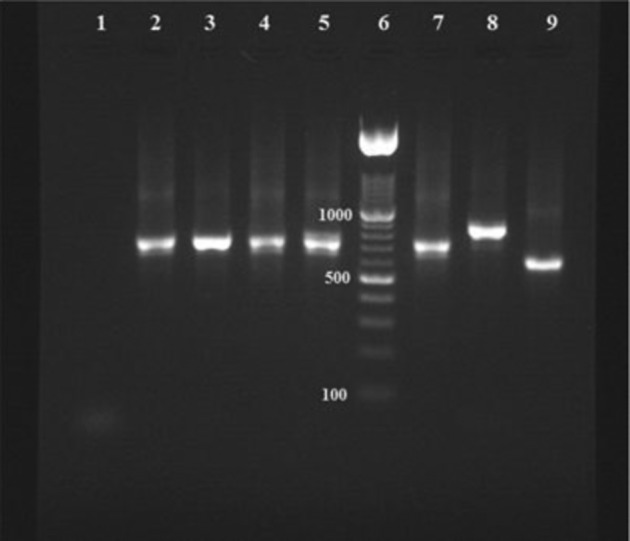
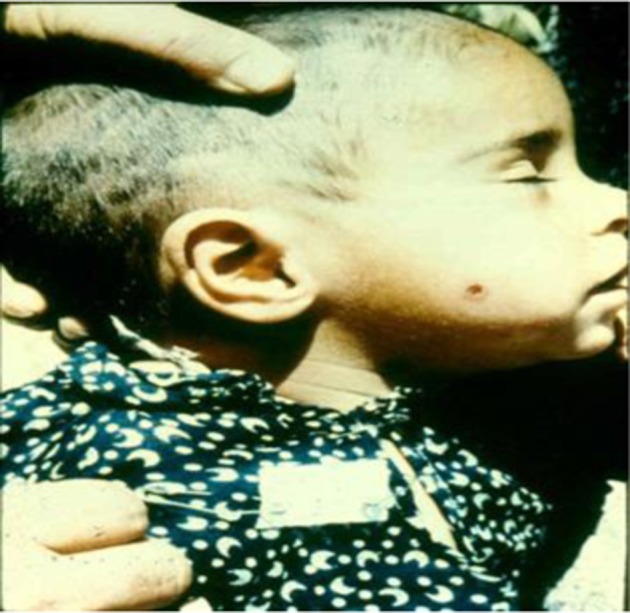
Visceral leishmaniasis (VL) is endemic in Northwest and southern Iran. Reports of cutaneous leishmaniasis (CL) in Northwest areas are rare, and its etiological agents are unknown. In the current study, we report six CL and two post kala-azar dermal leishmaniasis (PKDL) cases caused by Leishmania infantum from endemic areas of VL in the Northwest. Smears were made from skin lesions of 30 suspected patients in 2002-2011, and CL was determined by microscopy or culture. Leishmania spp. were identified by nested-PCR assay. The disease was confirmed in 20 out of 30 (66%) suspected patients by parasitological examinations. L. infantum was identified in eight and Leishmania major in 12 CL cases by nested-PCR. Cutaneous leishmaniasis patients infected with L. major had the history of travel to CL endemic areas. L. infantum antibodies were detected by direct agglutination test (DAT) at titers of 1:3200 in two cases with history of VL. Results of this study indicated that L. infantum is a causative agent of CL as well as PKDL in the VL endemic areas.
Figures
Similar articles
-
DNA-based detection of Leishmania and Crithidia species isolated from humans in cutaneous and post-kala-azar dermal leishmaniasis from Shiraz and Kharameh, southern Iran.J Vector Borne Dis. 2020 Jan-Mar;57(1):52-57. doi: 10.4103/0972-9062.309518. J Vector Borne Dis. 2020. PMID: 33818456
-
Canine visceral leishmaniasis: a comparative study of real-time PCR, conventional PCR, and direct agglutination on sera for the detection of Leishmania infantum infection.Vet Parasitol. 2013 Feb 18;192(1-3):83-90. doi: 10.1016/j.vetpar.2012.10.013. Epub 2012 Oct 26. Vet Parasitol. 2013. PMID: 23153824
-
PKDL and other dermal lesions in HIV co-infected patients with Leishmaniasis: review of clinical presentation in relation to immune responses.PLoS Negl Trop Dis. 2014 Nov 20;8(11):e3258. doi: 10.1371/journal.pntd.0003258. eCollection 2014. PLoS Negl Trop Dis. 2014. PMID: 25412435 Free PMC article. Review.
-
Population structures of Leishmania infantum and Leishmania tropica the causative agents of kala-azar in Southwest Iran.Parasitol Res. 2018 Nov;117(11):3447-3458. doi: 10.1007/s00436-018-6041-1. Epub 2018 Aug 13. Parasitol Res. 2018. PMID: 30105405
-
Visceral leishmaniasis in Iran: Review of the Epidemiological and Clinical Features.Iran J Parasitol. 2013 Jul;8(3):348-58. Iran J Parasitol. 2013. PMID: 24454426 Free PMC article. Review.
Cited by
-
Molecular Identification and Intra-species Variations among Leishmania infantum Isolated from Human and Canine Visceral Leishmaniasis in Iran.Iran J Parasitol. 2018 Oct-Dec;13(4):567-576. Iran J Parasitol. 2018. PMID: 30697310 Free PMC article.
-
[Generalized old world leishmaniasis: first Moroccan case in an immunocompetent adult?].Med Trop Sante Int. 2021 Nov 5;1(4):mtsi.2021.90. doi: 10.48327/mtsi.2021.90. eCollection 2021 Dec 31. Med Trop Sante Int. 2021. PMID: 35891918 Free PMC article. French.
-
An update on pharmacotherapy for leishmaniasis.Expert Opin Pharmacother. 2015 Feb;16(2):237-52. doi: 10.1517/14656566.2015.973850. Epub 2014 Oct 25. Expert Opin Pharmacother. 2015. PMID: 25346016 Free PMC article. Review.
-
Clinico-epidemiological analysis of Post kala-azar dermal leishmaniasis (PKDL) cases in India over last two decades: a hospital based retrospective study.BMC Public Health. 2015 Oct 26;15:1092. doi: 10.1186/s12889-015-2424-8. BMC Public Health. 2015. PMID: 26503551 Free PMC article.
-
The Geographical Distribution of Human Cutaneous and Visceral Leishmania Species Identified by Molecular Methods in Iran: A Systematic Review With Meta-Analysis.Front Public Health. 2021 Jun 25;9:661674. doi: 10.3389/fpubh.2021.661674. eCollection 2021. Front Public Health. 2021. PMID: 34249836 Free PMC article.
References
-
- World Health Organization. 2010. Report of a meeting of the WHO expert committee on the control of leishmaniases, 22–26 March 2010. Geneva.
-
- Reithinger R, Dujardin JD, Louzir H, Pirmez C, Alexander B, Brooker S. Cutaneous leishmaniasis. Lancet Infect Dis. 2007;7:581–96. - PubMed
-
- Edrissian GhH. Visceral leishmaniasis in Iran and the role of serological tests in diagnosis and epidemiological studies. Parasitology for 21st Century (ICOPA VIII) Izmir, Turkey: CAB International; 1996. pp. 63–78.
-
- Mohebali M, Javadian E, Yaghoobi-Ershadi MR, Akhavan AA, Hajjaran H, Abaei MR. Characterization of Leishmania infection in rodents from endemic areas of the Islamic Republic of Iran. East Mediterr Health J. 2004;10(4/5):591–9. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous