

Blood pressure and cholesterol control in hypertensive hypercholesterolemic patients: national health and nutrition examination surveys 1988-2010
- PMID: 23817481
- PMCID: PMC4066305
- DOI: 10.1161/CIRCULATIONAHA.112.000500
Blood pressure and cholesterol control in hypertensive hypercholesterolemic patients: national health and nutrition examination surveys 1988-2010
Abstract
Background: Hypertension doubles coronary heart disease (CHD) risk. Treating hypertension only reduces CHD risk ≈25%. Treating hypercholesterolemia in hypertensive patients reduces residual CHD risk >35%.
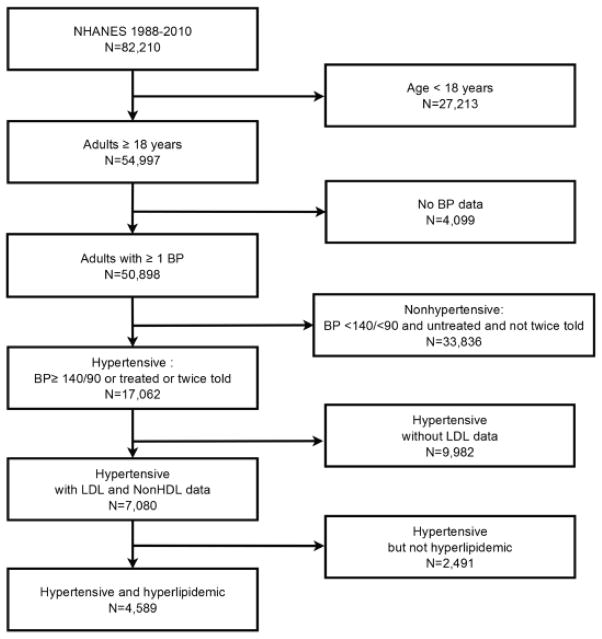
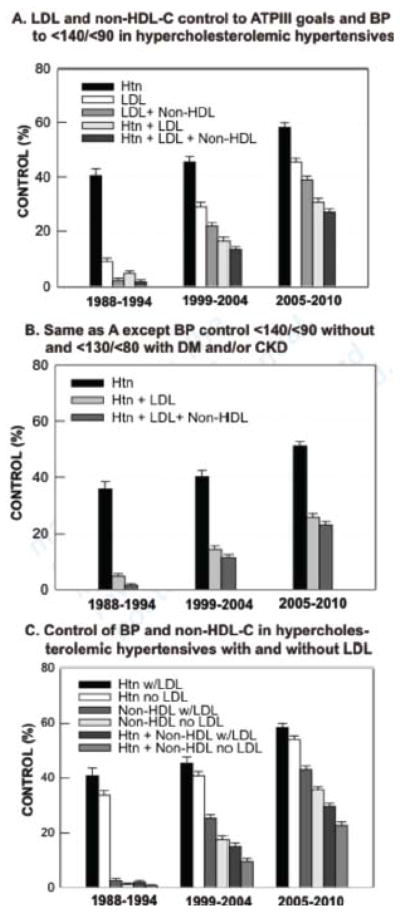
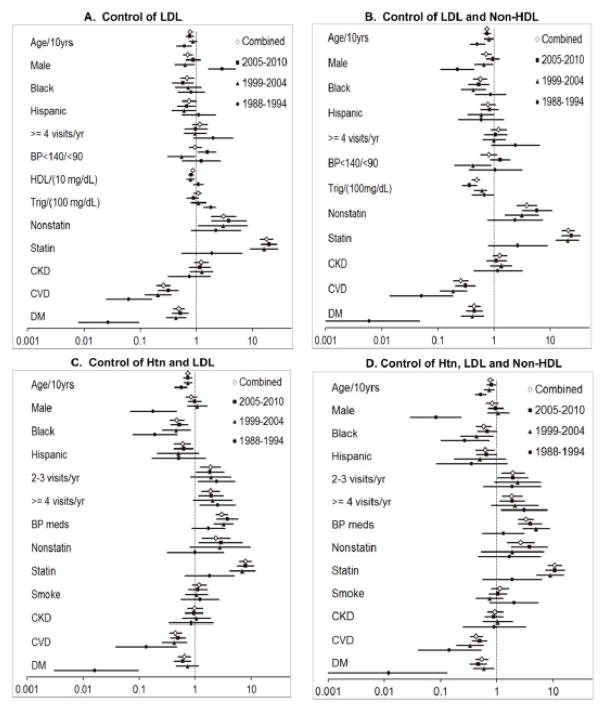
Methods and results: To assess progress in concurrent hypertension and hypercholesterolemia control, National Health and Nutrition Examination Surveys 1988 to 1994, 1999 to 2004, and 2005 to 2010 were analyzed. Hypertension was defined by blood pressure ≥140/≥90 mm Hg, current medication treatment, and 2-told hypertension status; blood pressure <140/<90 defined control. Hypercholesterolemia was defined by ATP III criteria based on 10-year CHD risk, low-density lipoprotein cholesterol (LDL-C), and non-high-density lipoprotein cholesterol; values below diagnostic thresholds defined control. Across surveys, 60.7% to 64.3% of hypertensives were hypercholesterolemic. From 1988 to 1994 to 2005 to 2010, control of LDL-C rose (9.2% [95% confidence interval (CI), 6.6%-11.9%] to 45.4% [95% CI, 42.6%-48.3%]), concomitant hypertension and LDL-C (5.0% [95% CI, 3.3%-6.7%] to 30.7% [95% CI, 27.9%-33.4%]), and combined hypertension, LDL-C, and non-high-density lipoprotein cholesterol (1.8% [95% CI, 0.4%-3.2%] to 26.9% [95% CI, 24.4%-29.5%]). By multivariable logistic regression, factors associated with concomitant hypertension, LDL-C, and non-high-density lipoprotein cholesterol control (odds ratio [95% CI]) were statin (10.7 [8.1-14.3]) and antihypertensive (3.32 [2.45-4.50]) medications, age (0.77 [0.69-0.88]/10-year increase), ≥2 healthcare visits/yr (1.90 [1.26-2.87]), black race (0.59 [0.44-0.80]), Hispanic ethnicity (0.62 [0.43-0.90]), cardiovascular disease (0.44 [0.34-0.56]), and diabetes mellitus (0.54 [0.42-0.70]).
Conclusions: Despite progress, opportunities for improving concomitant hypertension and hypercholesterolemia control persist. Prescribing antihypertensive and antihyperlipidemic medications to achieve treatment goals, especially for older, minority, diabetic, and cardiovascular disease patients, and accessing healthcare at least biannually could improve concurrent risk factor control and CHD prevention.
Keywords: cardiovascular diseases; coronary disease; hypercholesterolemia; hypertension; prevention & control.
Conflict of interest statement
Figures
References
-
- Egan BM, Zhao Y, Axon RN. US trends in prevalence, awareness, treatment, and control of hypertension, 1988–2008. JAMA. 2010;303:2043–2050. - PubMed
-
- Psaty BM, Lumly TM, Furberg CD, Schellenbaum G, Pahor M, Alderman MH, Weiss NS. Health outcomes associated with various antihypertensive therapies used as first-line agents: A network meta-analysis. JAMA. 2003;289:2534–2544. - PubMed
-
- Lewington S, Clarke R, Qizilbash N, Peto R, Collins R Prospective Studies Collaboration. Age-specific relevance of usual blood pressure to vascular mortality: a meta-analysis of individual data for one million adults in 61 prospective studies. Lancet. 2002;360:1903–1913. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
