

The effectiveness and safety of landiolol hydrochloride, an ultra-short-acting β1-blocker, in postoperative patients with supraventricular tachyarrhythmias: a multicenter, randomized, double-blind, placebo-controlled study
- PMID: 23818039
- PMCID: PMC3781301
- DOI: 10.1007/s40256-013-0035-2
The effectiveness and safety of landiolol hydrochloride, an ultra-short-acting β1-blocker, in postoperative patients with supraventricular tachyarrhythmias: a multicenter, randomized, double-blind, placebo-controlled study
Abstract
Background: Persistent postoperative supraventricular tachyarrhythmias (SVTs) increase cardiac burden and aggravate cardiac hemodynamics. Therefore, for patients in unstable conditions after surgery, prompt and sustained control of heart rate is essential. The importance of β-adrenoceptor antagonists (β-blockers) in controlling such postoperative atrial fibrillation or atrial flutter has been established, and the usefulness of ultra-short-acting β1-blockers with high β1 selectivity has been suggested based on their safety and efficacy under such circumstances.
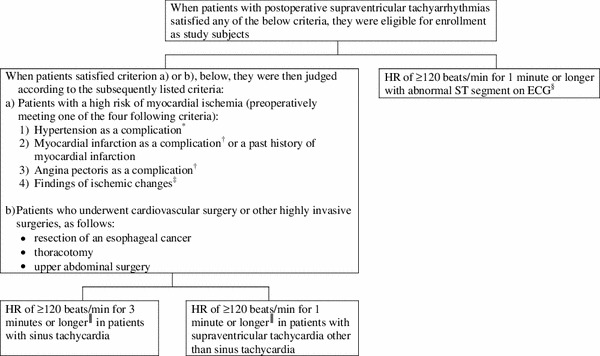
Objectives: Our objectives were to evaluate the effectiveness and safety of landiolol hydrochloride, an ultra-short-acting β1-selective blocker, in the treatment of postoperative SVT in patients with a high risk of myocardial ischemia, or in patients after highly invasive surgery, in a multicenter, randomized, double-blind, placebo-controlled, group-comparative study.
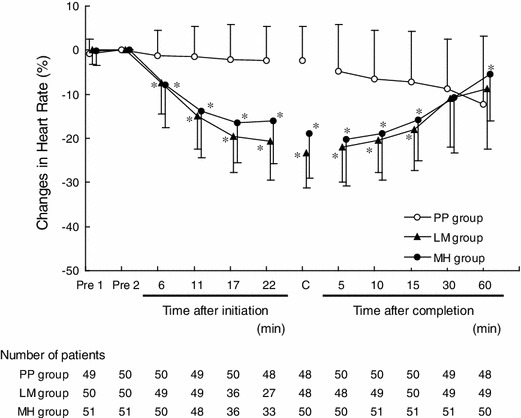
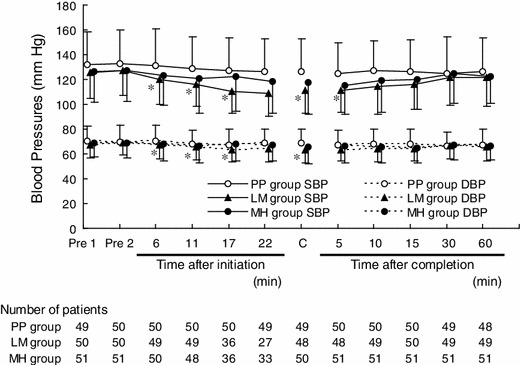
Methods: A total of 165 patients were randomly allocated to three groups and received LM or MH doses of landiolol hydrochloride or placebo. LM group: dose L (1-min loading dose at a rate of 0.03 mg/kg/min, followed by a 10-min infusion at 0.01 mg/kg/min) followed by dose M (1-min loading at a rate of 0.06 mg/kg/min, followed by a 10-min infusion at 0.02 mg/kg/min); MH group: dose M followed by dose H (1-min loading dose at a rate of 0.125 mg/kg/min, followed by a 10-min infusion at 0.04 mg/kg/min); placebo (PP) group: dose P (1-min loading dose at a rate of 0 mg/kg/min, followed by a 10-min infusion at 0 mg/kg/min) followed by another round of dose P. If the targeted heart-rate reduction was not obtained at the end of the first 10-min infusion, the higher dose was started. The primary endpoint was the percentage of patients who met the heart-rate reduction criteria (≥20 % reduction and <100 beats/min). The safety endpoint was the incidence of adverse events in each of the three groups.
Results: The percentages of patients who met the heart-rate reduction criteria (≥20 % reduction and <100 beats/min) were 0.0, 60.4, and 42.0 % in the PP, LM, and MH groups, respectively. There were significant differences in the LM and MH groups relative to the PP group, but there was no significant difference between the LM and MH groups. No significant difference was observed in the incidence of adverse events among the three groups: 29.6 % in the PP group, 45.5 % in the LM group, and 43.1 % in the MH group.
Conclusion: Landiolol hydrochloride is effective and safe for patients with postoperative SVT.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
