

The association of neonatal dacryocystoceles and infantile dacryocystitis with nasolacrimal duct cysts (an American Ophthalmological Society thesis)
- PMID: 23818736
- PMCID: PMC3671363
The association of neonatal dacryocystoceles and infantile dacryocystitis with nasolacrimal duct cysts (an American Ophthalmological Society thesis)
Abstract
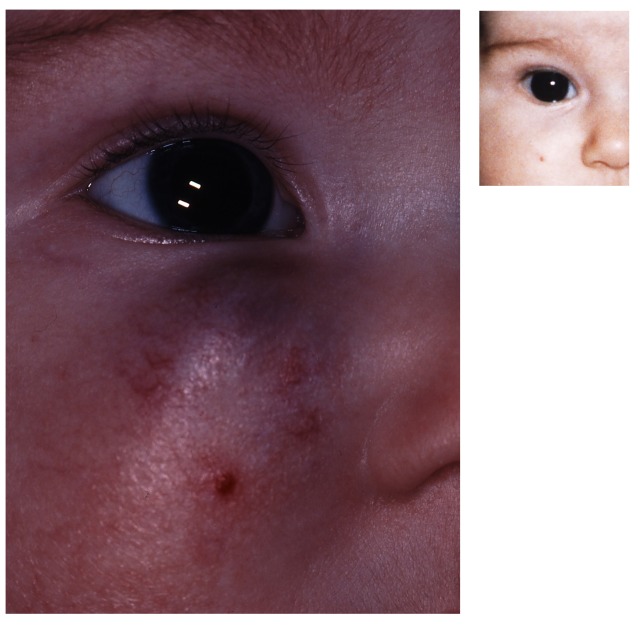
Purpose: To investigate whether neonatal dacryocystoceles and dacryocystitis are associated with nasolacrimal duct cysts, and to report the outcomes of treatment of these disorders.
Methods: This was a retrospective medical record review of two groups of infants with nasolacrimal duct (NLD) obstruction. The first group had dacryocystoceles with or without dacryocystitis. The second group had NLD obstruction with symptoms severe enough to require early NLD probing. All of the patients underwent NLD probing and nasal endoscopy. When present, NLD cysts were removed.
Results: In the first group, 33 infants had dacryocystoceles. Acute dacryocystitis was present in 16 patients, 12 had noninfected dacryocystoceles that did not resolve, and 5 had dacryocystoceles that resolved but severe symptoms persisted. All of the patients had NLD cysts that were surgically removed. The symptoms resolved after surgery in 31 patients (94%). In the second group, 27 infants less than 6 months old without dacryocystoceles underwent early NLD probing and endoscopy due to severity of symptoms. Twelve (44%) of these patients had NLD cysts. The symptoms resolved in 11 (92%) of 12 patients following NLD probing and cyst removal.
Conclusions: Neonatal dacryocystoceles are almost always associated with NLD cysts. The success rate of NLD probing and endoscopic cyst removal in these patients is excellent. Nasolacrimal duct cysts also are present in many young infants with severe symptoms of NLD obstruction. Nasal endoscopy is an important adjunct to the management of these infants.
Figures














References
-
- Guerry D, III, Kendig EL., Jr Congenital impatency of the nasolacrimal duct. Arch Ophthalmol. 1948;39(2):193–201. - PubMed
-
- MacEwen CJ, Young JDH. Epiphora during the first year of life. Eye (Lond) 1991;5(Pt 5):596–600. - PubMed
-
- MacEwen CJ, Phillips MG, Young JDH. Value of bacterial culturing in the course of congenital nasolacrimal duct (NLD) obstruction. J Pediatr Ophthalmol Strabismus. 1994;31(4):246–250. - PubMed
-
- Harris GJ, DiClementi D. Congenital dacryocystocele. Arch Ophthalmol. 1982;100(11):1763–1765. - PubMed
-
- Sullivan TJ, Clarke MP, Morin JD, Pashby RC. Management of congenital dacryocystocoele. Aust N Z J Ophthalmol. 1992;20(2):105–108. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
