

Vertebral compression fractures: a review of current management and multimodal therapy
- PMID: 23818797
- PMCID: PMC3693826
- DOI: 10.2147/JMDH.S31659
Vertebral compression fractures: a review of current management and multimodal therapy
Abstract
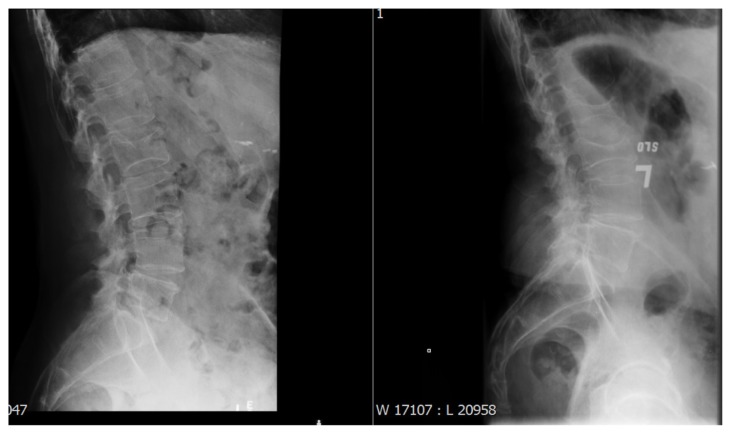
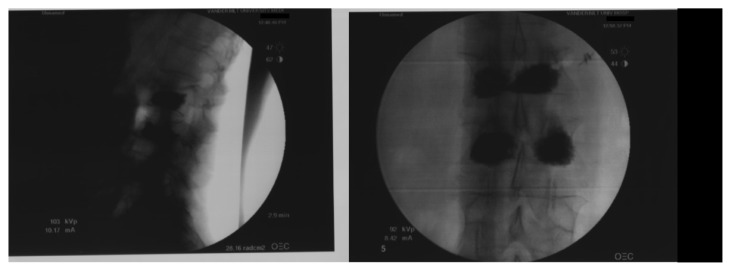
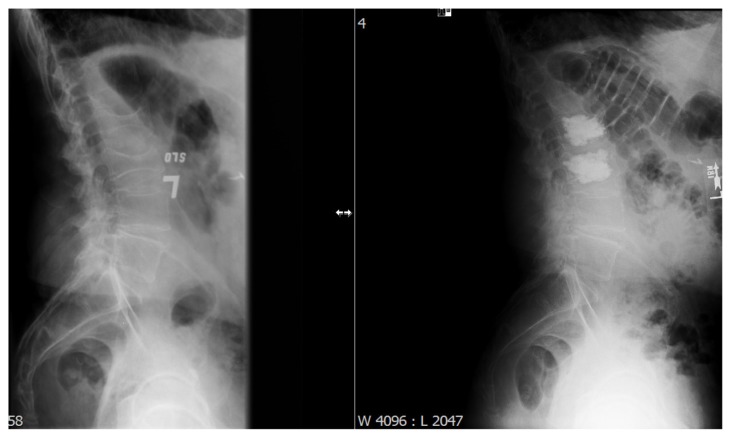
Vertebral compression fractures are a prevalent disease affecting osteoporotic patients. When symptomatic, they cause significant pain and loss of function and have a high public health impact. In this paper we outline the diagnosis and management of these patients, with evidence-based review of treatment outcomes for the various therapeutic options. Diagnosis involves a clinical history focusing on the nature of the patient's pain as well as various imaging studies. Management is multimodal in nature and starts with conservative therapy consisting of analgesic medication, medication for osteoporosis, physical therapy, and bracing. Patients who are refractory to conservative management may be candidates for vertebral augmentation through either vertebroplasty or kyphoplasty.
Keywords: bracing; kyphoplasty; osteoporosis; vertebral compression fractures; vertebroplasty.
Figures


References
-
- Ensrud KE, Schousboe JT. Clinical practice. Vertebral fractures. N Engl J Med. 2011;364(17):1634–1642. - PubMed
-
- Fink HA, Milavetz DL, Palermo L, et al. What proportion of incident radiographic vertebral deformities is clinically diagnosed and vice versa? J Bone Miner Res. 2005;20(7):1216–1222. - PubMed
-
- Francis RM, Baillie SP, Chuck AJ, et al. Acute and long-term management of patients with vertebral fractures. QJM. 2004;97(2):63–74. - PubMed
-
- Cooper C. Epidemiology and public health impact of osteoporosis. Baillieres Clin Rheumatol. 1993;7(3):459–477. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
