

Care in specialist medical and mental health unit compared with standard care for older people with cognitive impairment admitted to general hospital: randomised controlled trial (NIHR TEAM trial)
- PMID: 23819964
- PMCID: PMC3698942
- DOI: 10.1136/bmj.f4132
Care in specialist medical and mental health unit compared with standard care for older people with cognitive impairment admitted to general hospital: randomised controlled trial (NIHR TEAM trial)
Abstract
Objective: To develop and evaluate a best practice model of general hospital acute medical care for older people with cognitive impairment.
Design: Randomised controlled trial, adapted to take account of constraints imposed by a busy acute medical admission system.
Setting: Large acute general hospital in the United Kingdom.
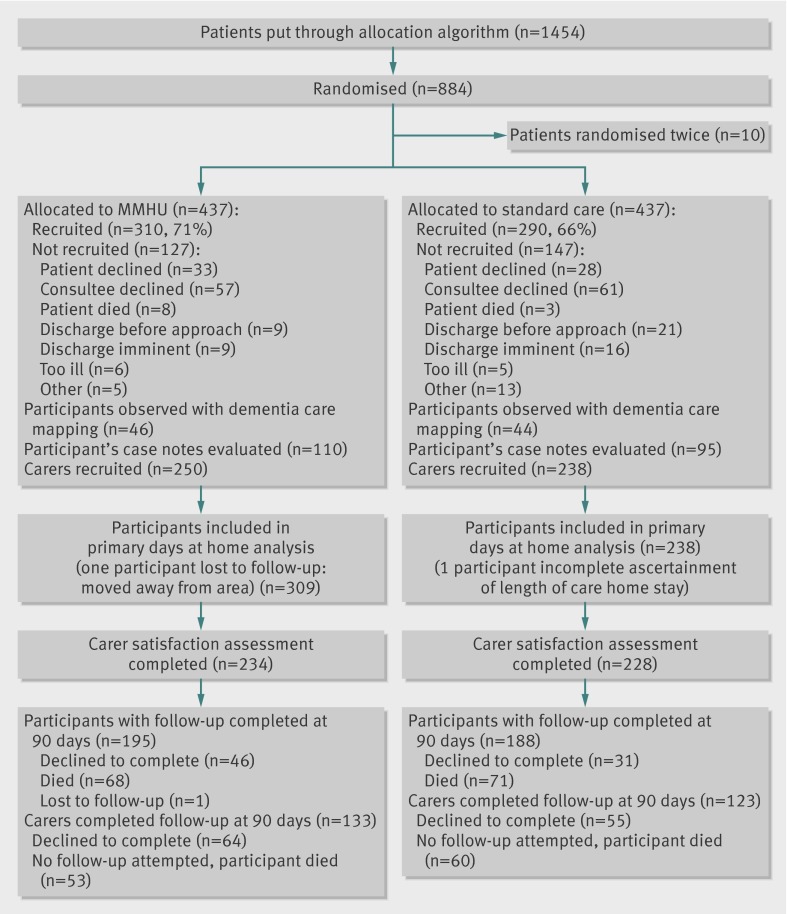
Participants: 600 patients aged over 65 admitted for acute medical care, identified as "confused" on admission.
Interventions: Participants were randomised to a specialist medical and mental health unit, designed to deliver best practice care for people with delirium or dementia, or to standard care (acute geriatric or general medical wards). Features of the specialist unit included joint staffing by medical and mental health professionals; enhanced staff training in delirium, dementia, and person centred dementia care; provision of organised purposeful activity; environmental modification to meet the needs of those with cognitive impairment; delirium prevention; and a proactive and inclusive approach to family carers.
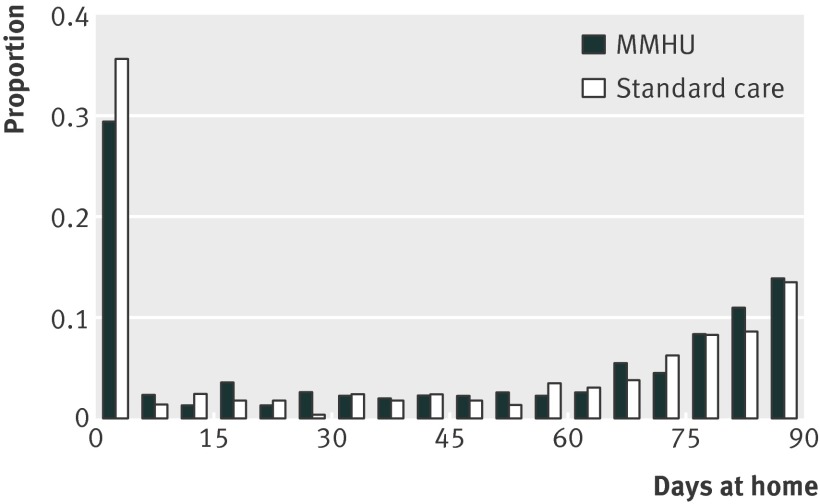
Primary outcome: number of days spent at home over the 90 days after randomisation.
Secondary outcomes: structured non-participant observations to ascertain patients' experiences; satisfaction of family carers with hospital care. When possible, outcome assessment was blind to allocation.
Results: There was no significant difference in days spent at home between the specialist unit and standard care groups (median 51 v 45 days, 95% confidence interval for difference -12 to 24; P=0.3). Median index hospital stay was 11 versus 11 days, mortality 22% versus 25% (-9% to 4%), readmission 32% versus 35% (-10% to 5%), and new admission to care home 20% versus 28% (-16% to 0) for the specialist unit and standard care groups, respectively. Patients returning home spent a median of 70.5 versus 71.0 days at home (-6.0 to 6.5). Patients on the specialist unit spent significantly more time with positive mood or engagement (79% v 68%, 2% to 20%; P=0.03) and experienced more staff interactions that met emotional and psychological needs (median 4 v 1 per observation; P<0.001). More family carers were satisfied with care (overall 91% v 83%, 2% to 15%; P=0.004), and severe dissatisfaction was reduced (5% v 10%, -10% to 0%; P=0.05).
Conclusions: Specialist care for people with delirium and dementia improved the experience of patients and satisfaction of carers, but there were no convincing benefits in health status or service use. Patients' experience and carers' satisfaction might be more appropriate measures of success for frail older people approaching the end of life.
Trial registration: Clinical Trials NCT01136148.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures
References
-
- Royal College of Psychiatrists. Who cares wins. RCP, 2005. www.rcpsych.ac.uk/PDF/WhoCaresWins.pdf.
-
- Holmes J, House A. Psychiatric illness predicts poor outcome after surgery for hip fracture: a prospective cohort study. Psychol Med 2000;30:921-9. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous