

Low-grade salivary duct carcinoma or low-grade intraductal carcinoma? Review of the literature
- PMID: 23821212
- PMCID: PMC3712095
- DOI: 10.1007/s12105-013-0460-1
Low-grade salivary duct carcinoma or low-grade intraductal carcinoma? Review of the literature
Abstract
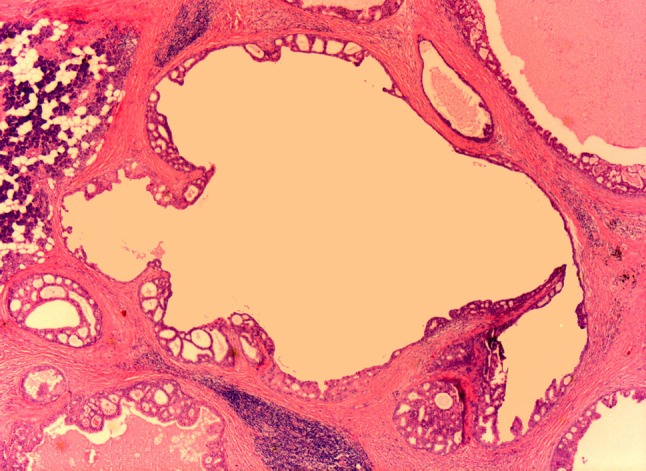
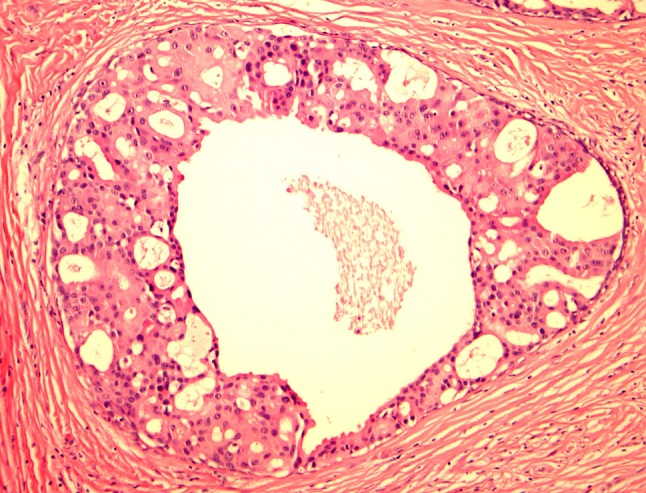
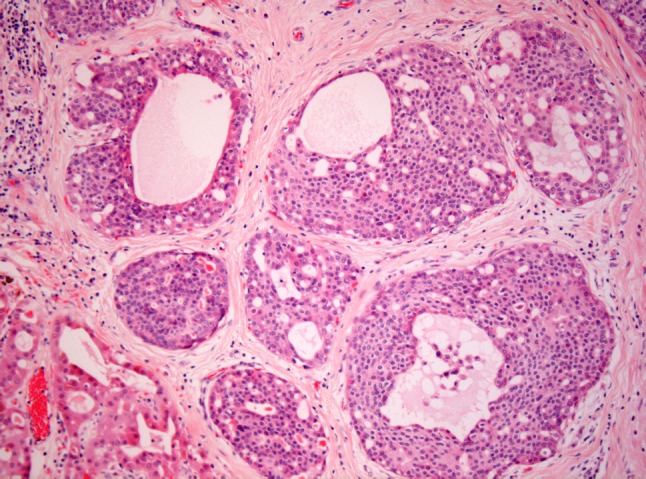
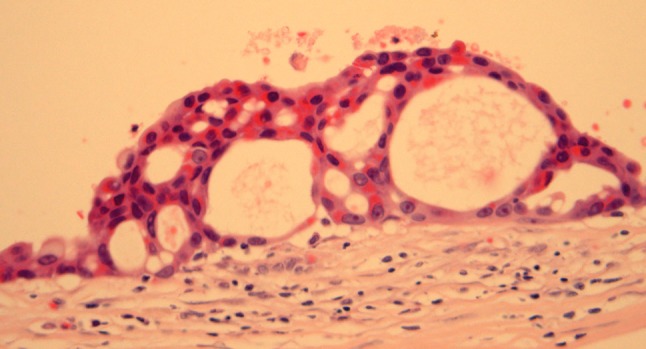
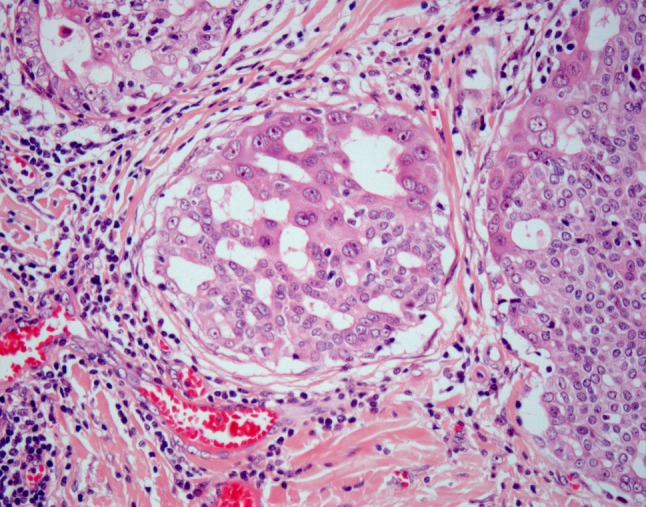
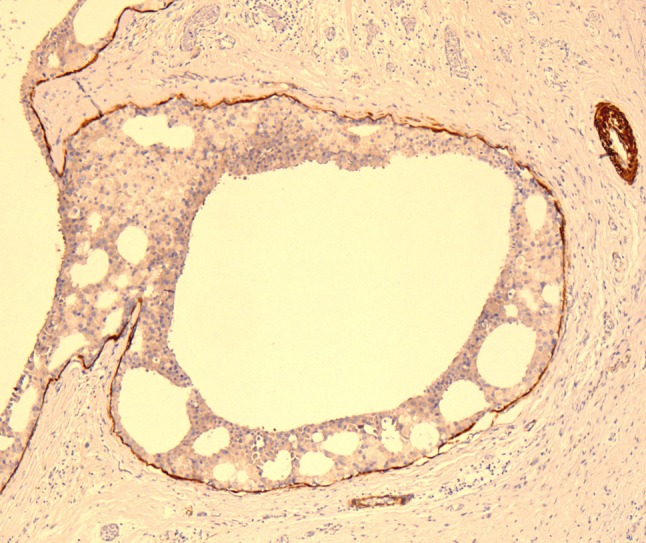
Low-grade salivary duct carcinoma (LG-SDC) is a rare neoplasm characterized by predominant intraductal growth, luminal ductal phenotype, bland microscopic features, and favorable clinical behavior with an appearance reminiscent of florid to atypical ductal hyperplasia to low grade intraductal breast carcinoma. LG-SDC is composed of multiple cysts, cribriform architecture with "Roman Bridges", "pseudocribriform" proliferations with floppy fenestrations or irregular slits, micropapillae with epithelial tufts, fibrovascular cores, and solid areas. Most of the tumor cells are small to medium sized with pale eosinophilic cytoplasm, and round to oval nuclei, which may contain finely dispersed or dark condensed chromatin. Foci of intermediate to high grade atypia, and invasive carcinoma or micro-invasion have been reported in up to 23 % of cases. The neoplastic cells have a ductal phenotype with coexpression of keratins and S100 protein and are surrounded by a layer of myoepithelial cells in non-invasive cases. The main differential diagnosis of LG-SDC includes cystadenoma, cystadenocarcinoma, sclerosing polycystic adenosis, salivary duct carcinoma in situ/high-grade intraductal carcinoma, and papillary-cystic variant of acinic cell carcinoma. There is no published data supporting the continuous classification of LG-SDC as a variant of cystadenocarcinoma. Given that most LG-SDC are non-invasive neoplasms; the terms "cribriform cystadenocarcinoma" and LG-SDC should be replaced by "low-grade intraductal carcinoma" (LG-IDC) of salivary gland or "low-grade intraductal carcinoma with areas of invasive carcinoma" in those cases with evidence of invasive carcinoma.
Figures


References
-
- Brandwein-Gensler M, Gnepp DR. Low-grade cribriform cystadenocarcinoma. In: Barnes L, Eveson JW, Reichart P, et al editors. Pathology and Genetics Head and Neck Tumors. Lyon: IARC Press; 2005; 233.
-
- Brandwein-Gensler M, Hille J, Wang BY, et al. Low-grade salivary duct carcinoma: description of 16 cases. Am J Surg Pathol. 2004;28:1040–1044. doi: 10.1097/01.pas.0000128662.66321.be. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
