

Multi-Institutional Sharing of Electronic Health Record Data to Assess Childhood Obesity
- PMID: 23823186
- PMCID: PMC3688837
- DOI: 10.1371/journal.pone.0066192
Multi-Institutional Sharing of Electronic Health Record Data to Assess Childhood Obesity
Abstract
Objective: To evaluate the validity of multi-institutional electronic health record (EHR) data sharing for surveillance and study of childhood obesity.
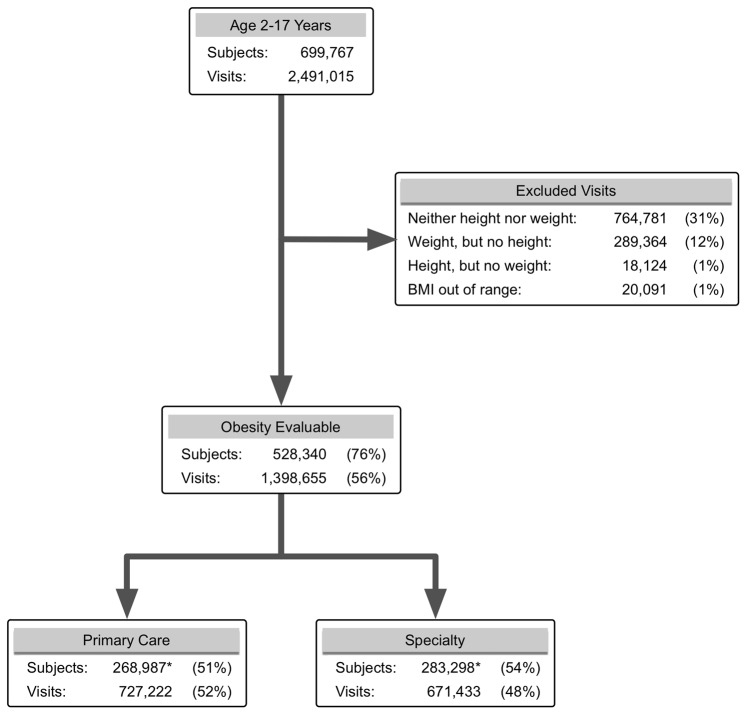
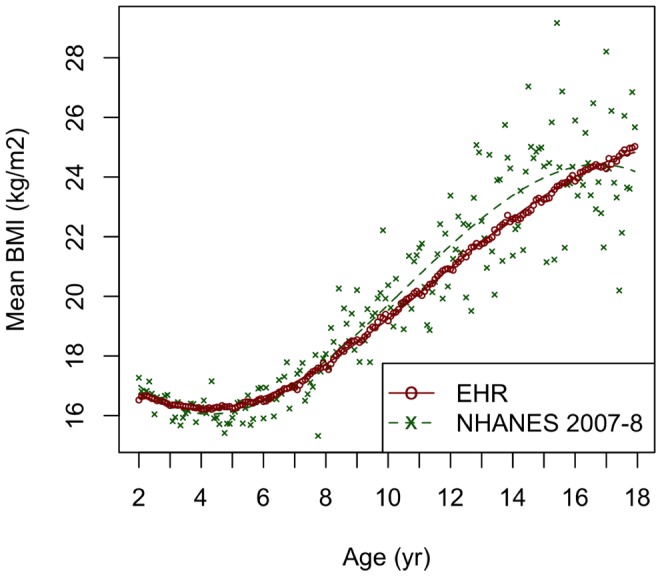
Methods: We conducted a non-concurrent cohort study of 528,340 children with outpatient visits to six pediatric academic medical centers during 2007-08, with sufficient data in the EHR for body mass index (BMI) assessment. EHR data were compared with data from the 2007-08 National Health and Nutrition Examination Survey (NHANES).
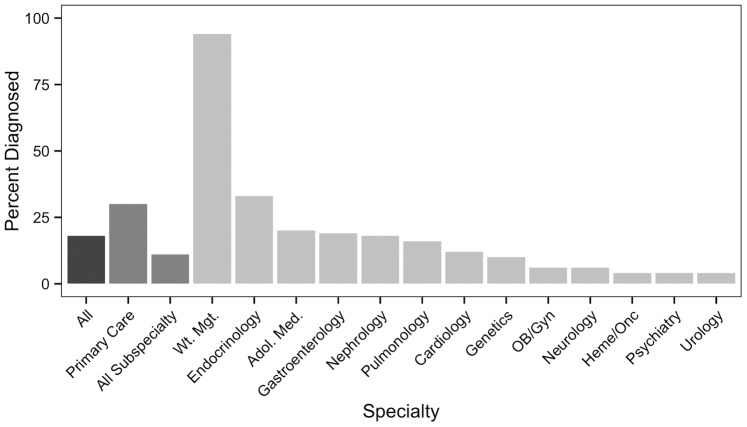
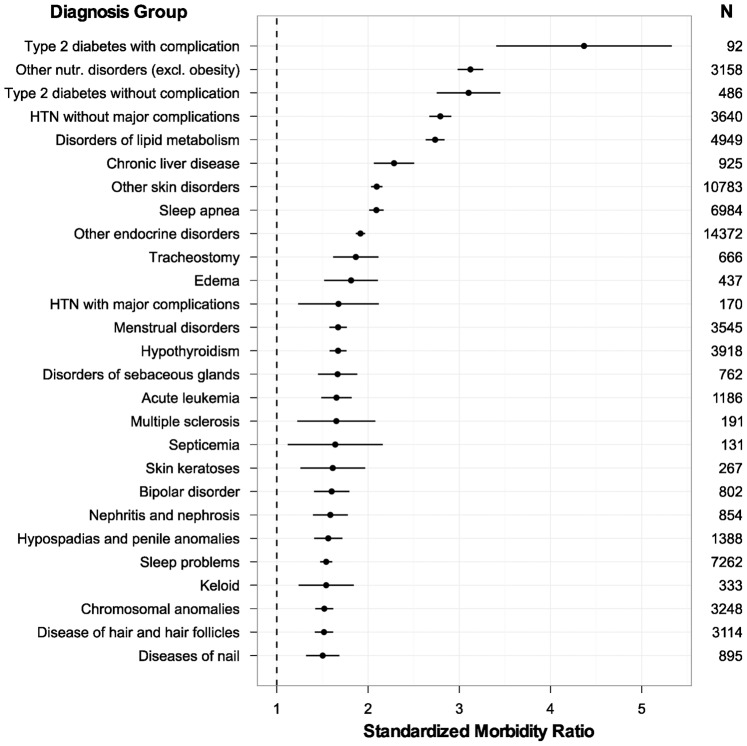
Results: Among children 2-17 years, BMI was evaluable for 1,398,655 visits (56%). The EHR dataset contained over 6,000 BMI measurements per month of age up to 16 years, yielding precise estimates of BMI. In the EHR dataset, 18% of children were obese versus 18% in NHANES, while 35% were obese or overweight versus 34% in NHANES. BMI for an individual was highly reliable over time (intraclass correlation coefficient 0.90 for obese children and 0.97 for all children). Only 14% of visits with measured obesity (BMI ≥95%) had a diagnosis of obesity recorded, and only 20% of children with measured obesity had the diagnosis documented during the study period. Obese children had higher primary care (4.8 versus 4.0 visits, p<0.001) and specialty care (3.7 versus 2.7 visits, p<0.001) utilization than non-obese counterparts, and higher prevalence of diverse co-morbidities. The cohort size in the EHR dataset permitted detection of associations with rare diagnoses. Data sharing did not require investment of extensive institutional resources, yet yielded high data quality.
Conclusions: Multi-institutional EHR data sharing is a promising, feasible, and valid approach for population health surveillance. It provides a valuable complement to more resource-intensive national surveys, particularly for iterative surveillance and quality improvement. Low rates of obesity diagnosis present a significant obstacle to surveillance and quality improvement for care of children with obesity.
Conflict of interest statement
Figures
References
-
- National Research Council, Institute of Medicine (2004) Children’s Health, the Nation’s Wealth: Assessing and Improving Child Health. Washington, DC: National Academies Press.
-
- Hsiao CJ, Hing E (2012) Use and characteristics of electronic health record systems among office-based physician practices: United States, 2001–2012. NCHS data brief: 1–8. - PubMed
-
- Centers for Medicare and Medicaid Services H (2010) Medicare and Medicaid programs; electronic health record incentive program. Final rule. Federal register 75: 44313–44588. - PubMed
-
- Blumenthal D, Tavenner M (2010) The “meaningful use” regulation for electronic health records. The New England journal of medicine 363: 501–504. - PubMed
-
- Olsen L, Aisner D, McGinnis JM (2007) The Learning Healthcare System. Washington, DC: National Academies Press. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
