

A comparative study between the imaging system and the optical tracking system in proton therapy at CNAO
- PMID: 23824116
- PMCID: PMC3700512
- DOI: 10.1093/jrr/rrt043
A comparative study between the imaging system and the optical tracking system in proton therapy at CNAO
Abstract
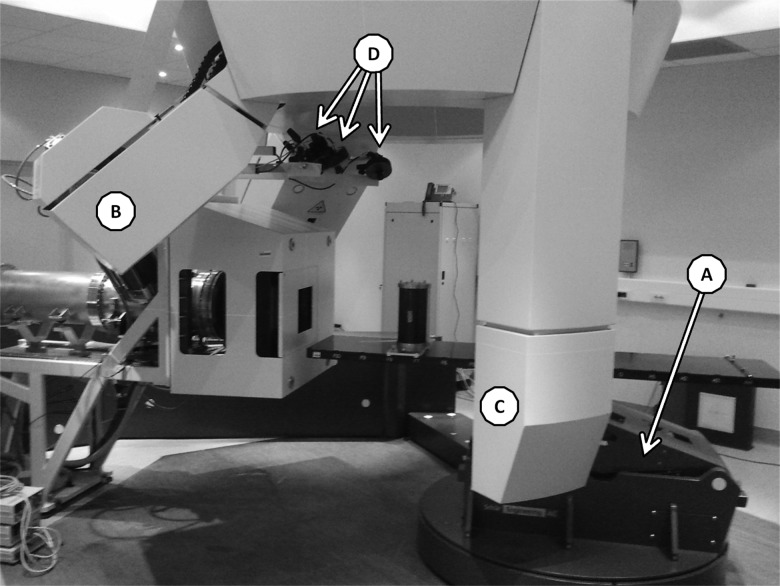
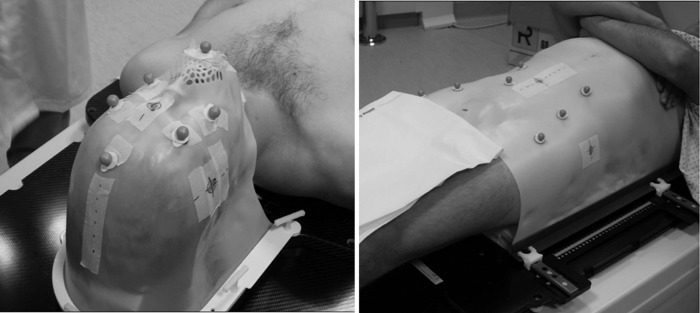
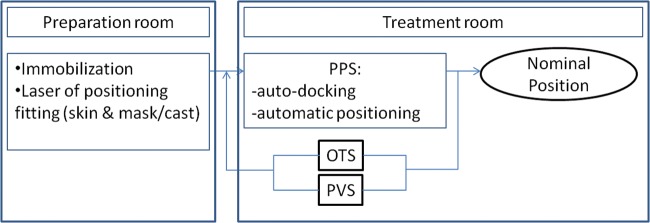
The synergy between in-room imaging and optical tracking, in co-operation with highly accurate robotic patient handling represents a concept for patient-set-up which has been implemented at CNAO (Centro Nazionale di Adroterapia Oncologica). In-room imaging is based on a double oblique X-ray projection system; optical tracking consists of the detection of the position of spherical markers placed directly on the patient's skin or on the immobilization devices. These markers are used as external fiducials during patient positioning and dose delivery. This study reports the results of a comparative analysis between in-room imaging and optical tracking data for patient positioning within the framework of high-precision particle therapy. Differences between the optical tracking system (OTS) and the imaging system (IS) were on average within the expected localization accuracy. On the first 633 fractions for head and neck (H&N) set-up procedures, the corrections applied by the IS, after patient positioning using the OTS only, were for the mostly sub-millimetric regarding the translations (0.4 ± 1.1 mm) and sub-gradual regarding the rotations (0.0° ± 0.8°). On the first 236 fractions for pelvis localizations the amplitude of the corrections applied by the IS after preliminary optical set-up correction were moderately higher and more dispersed (translations: 1.3 ± 2.9 mm, rotations 0.1 ± 0.9°). Although the indication of the OTS cannot replace information provided by in-room imaging devices and 2D-3D image registration, the reported data show that OTS preliminary correction might greatly support image-based patient set-up refinement and also provide a secondary, independent verification system for patient positioning.
Keywords: IGRT; head and neck; optical tracking system; particle therapy; patient positioning; pelvis localizations.
Figures
References
-
- Jaffray D. Image-guided radiotherapy: from current concept to future perspectives. Nat Rev Clin Oncol. 2012;9:688–99. - PubMed
-
- Shirato H, Shimizu S, Kunieda T, et al. Physical aspects of a real-time tumor-tracking system for gated radiotherapy. Int J Radiat Oncol Biol Phys. 2000;48:1187–95. - PubMed
-
- Shirato H, Shimizu S, Shimizu T, et al. Real-time tumour-tracking radiotherapy. Lancet. 1999;353:1331–2. - PubMed
-
- Riboldi M, Orecchia R, Baroni G. Real-time tumour tracking in particle therapy: technological developments and future perspectives. Lancet Oncol. 2012;13:e383–91. - PubMed
-
- Poulit J, Bani-Hashemi A, Chen J, et al. Low-dose megavoltage cone-beam CT for radiation therapy. Int J Radiat Oncol Biol Phys. 2005;61:552–60. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
