

Catheter ablation of idiopathic premature ventricular contractions and ventricular tachycardias originating from right ventricular septum
- PMID: 23825610
- PMCID: PMC3692551
- DOI: 10.1371/journal.pone.0067038
Catheter ablation of idiopathic premature ventricular contractions and ventricular tachycardias originating from right ventricular septum
Abstract
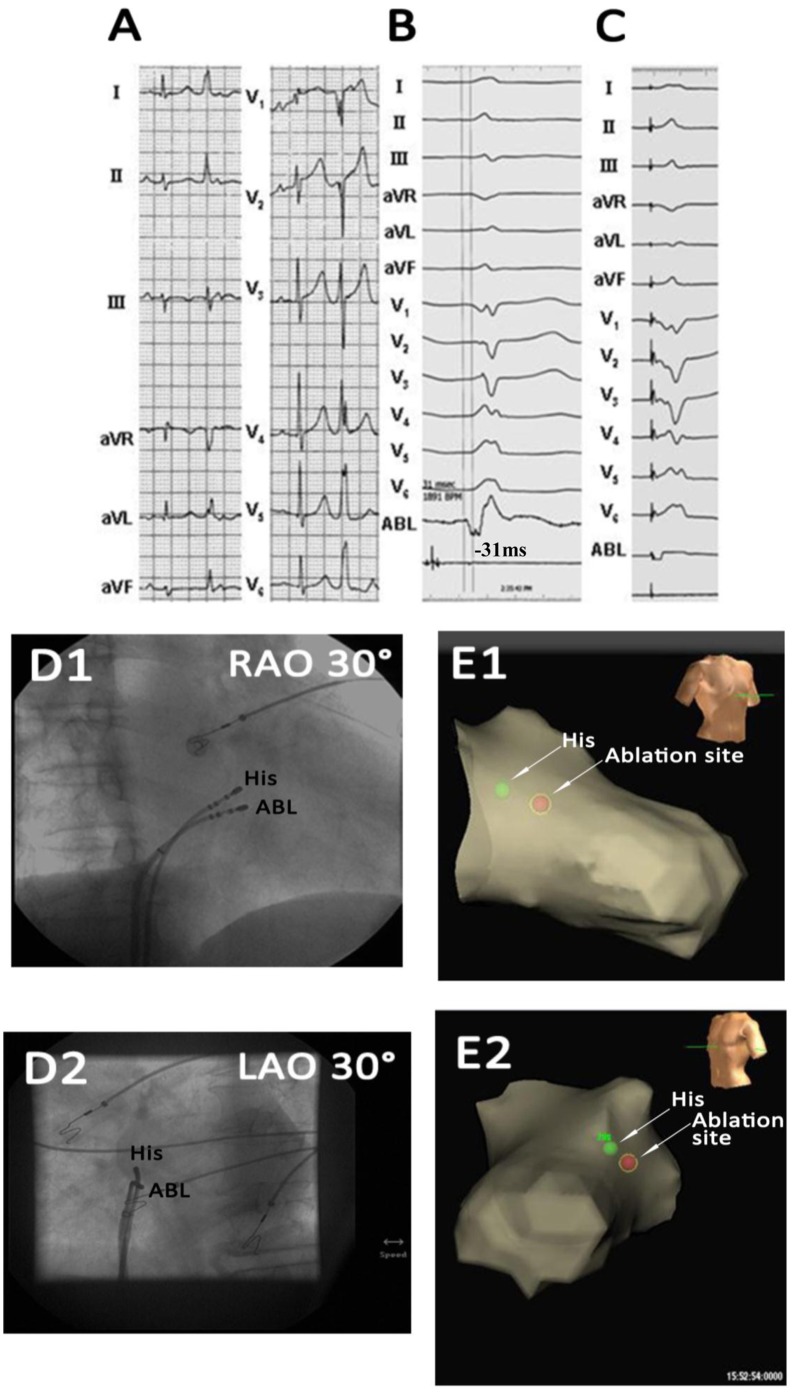
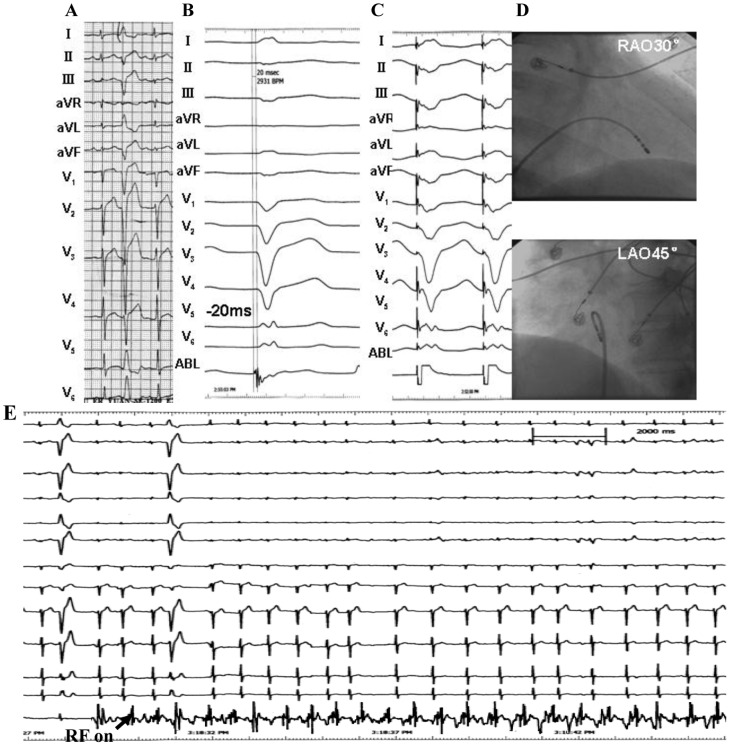
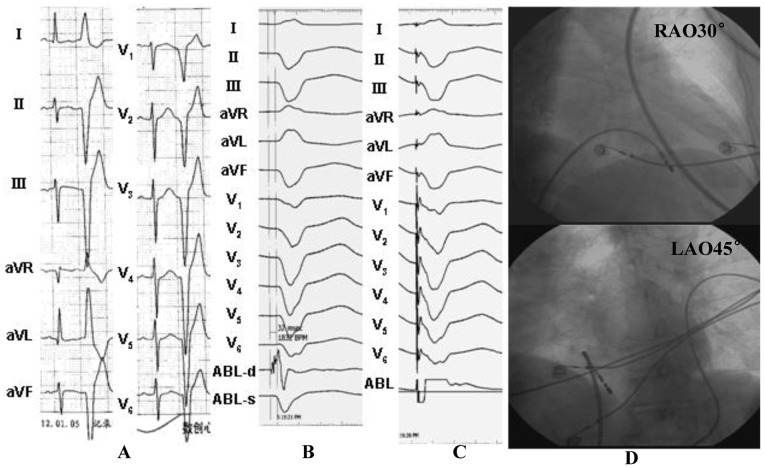
Background: Idiopathic premature ventricular contractions (PVCs) and ventricular tachycardias (IVTs) originating from the subtricuspid septum and near the His bundle have been reported. However, little is known about the prevalence, distribution, electrocardiographic characteristics and the efficacy of radiofrequency catheter ablation (RFCA) for the ventricular arrhythmias arising from the right ventricular (RV) septum. This study aimed to investigate electrocardiographic characteristics and effects of RFCA for patients with symptomatic PVCs/IVTs, originating from the different portions of the RV septum.
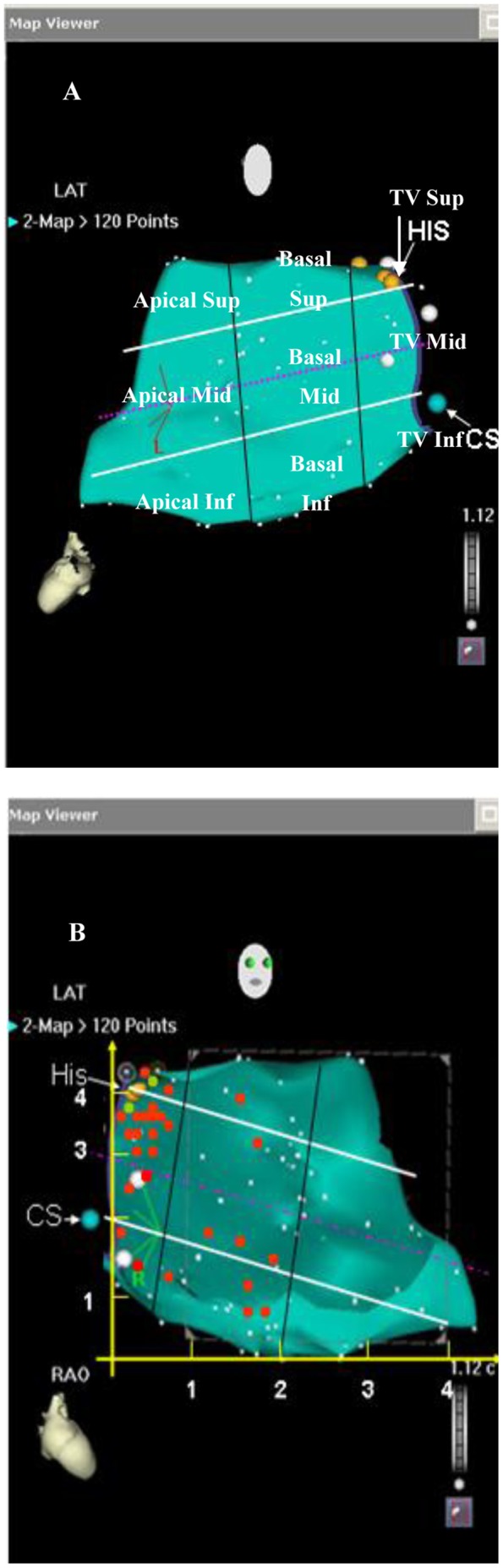
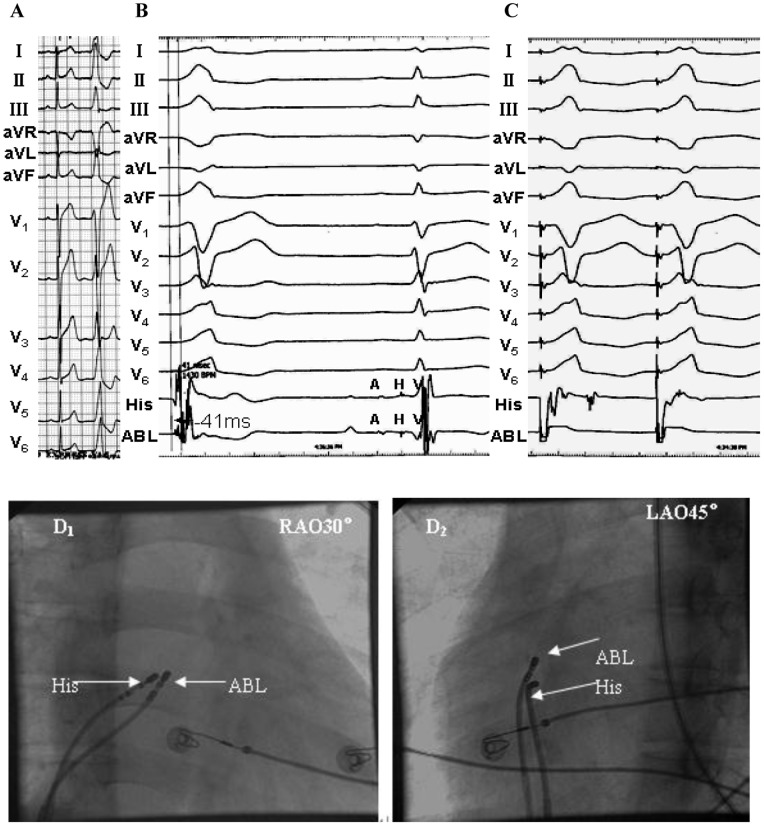
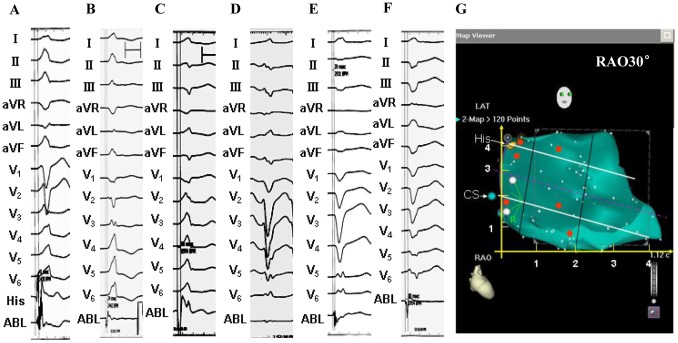
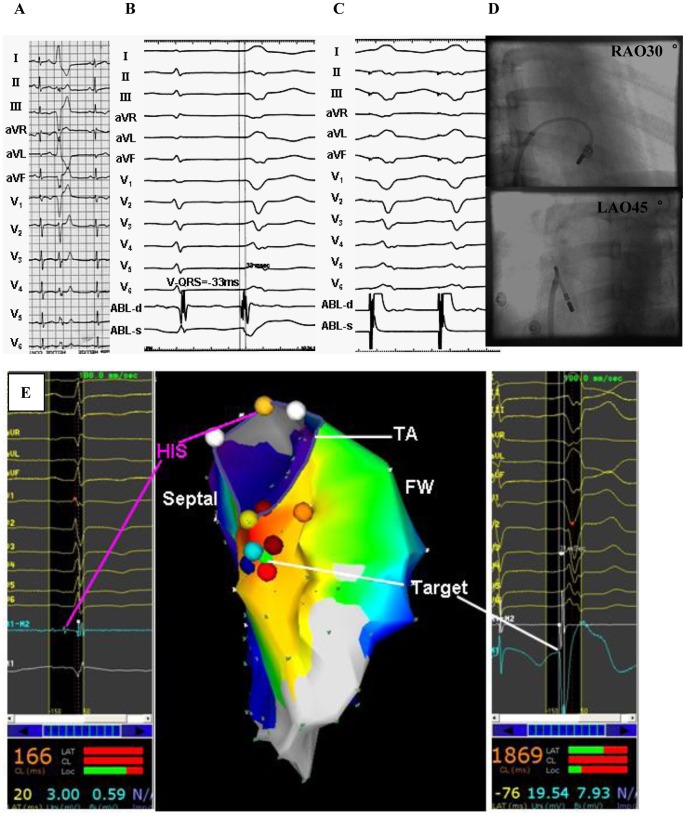
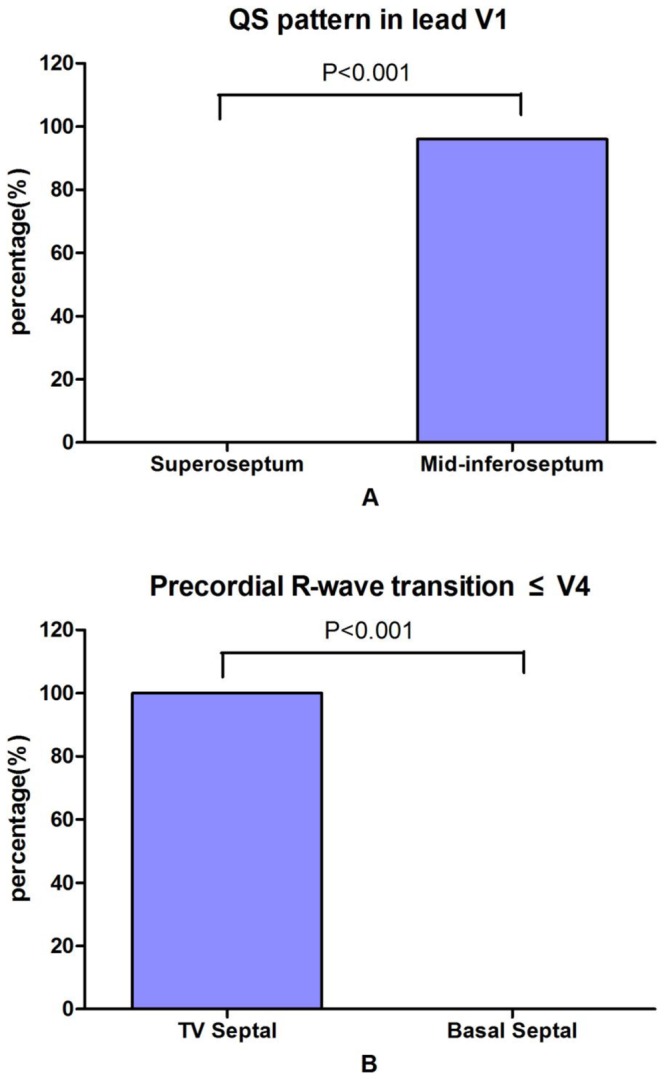
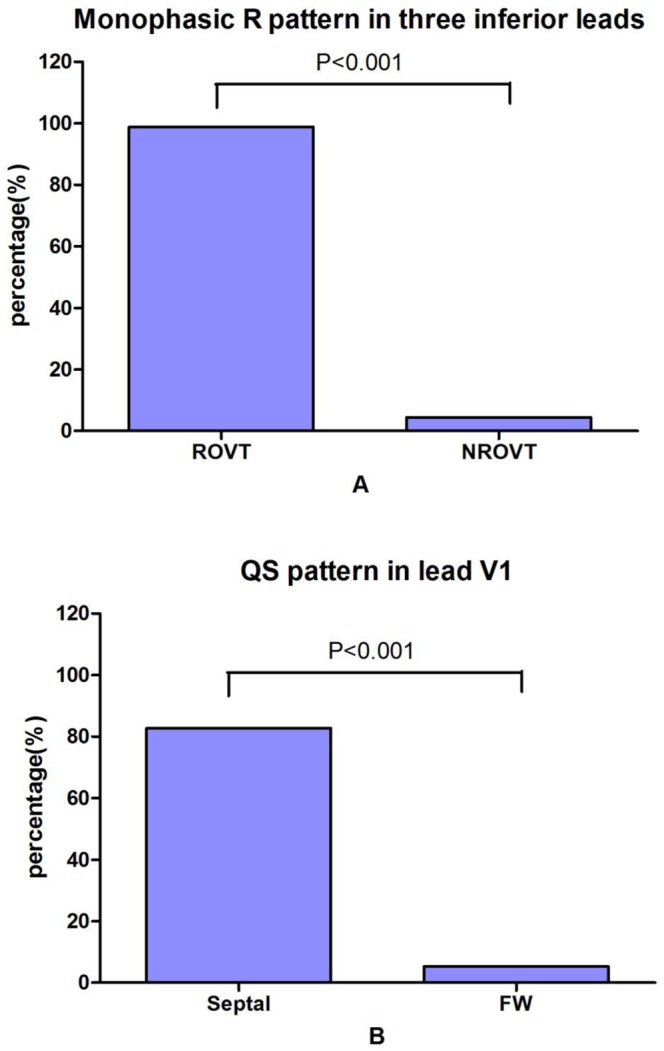
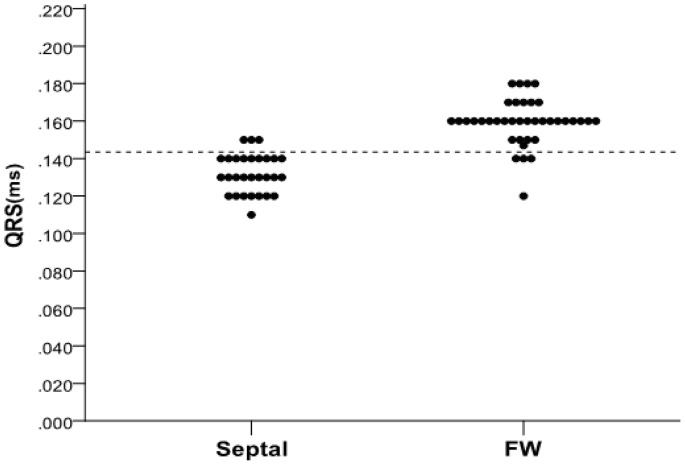
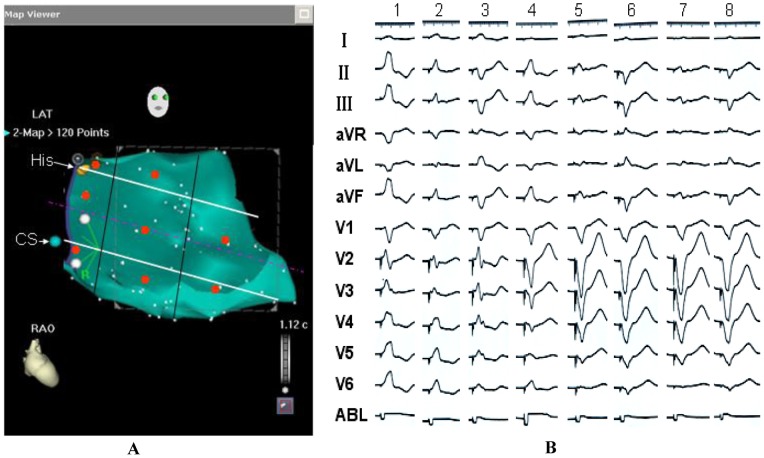
Methodology/principal findings: Characteristics of body surface electrocardiogram and electrophysiologic recordings were analyzed in 29 patients with symptomatic PVCs/IVTs originating from the RV septum. Among 581 patients with PVCs/IVTs, the incidence of ventricular arrhythmias originating from the RV septum was 5%. Twenty (69%) had PVCs/IVTs from the septal portion of the tricuspid valvular RV region (3 from superoseptum, 15 from midseptum, 2 from inferoseptum), and 9 (31%) from the septal portion of the basal RV (1 from superoseptum, 4 from midseptum, 4 from inferoseptum). There were different characteristics of ECG of PVCs/VT originating from the different portions of the RV septum. Twenty-seven of 29 patients with PVCs/IVTs arising from the RV septum were successfully ablated (93.1% acute success).
Conclusions/significance: ECG characteristics of PVCs/VTs originating from the different portions of the RV septum are different, and can help regionalize the origin of these arrhythmias. The septal portion of the tricuspid valvular RV region was the preferential site of origin. RFCA was effective and safe for the PVCs/IVTs arising from the RV septum.
Conflict of interest statement
Figures
Similar articles
-
Catheter ablation of idiopathic premature ventricular contractions and ventricular tachycardias originating from the vicinity of endocardial and epicardial mitral annulus.PLoS One. 2013 Nov 27;8(11):e80777. doi: 10.1371/journal.pone.0080777. eCollection 2013. PLoS One. 2013. PMID: 24312241 Free PMC article.
-
Idiopathic premature ventricular contractions and ventricular tachycardias originating from the vicinity of tricuspid annulus: results of radiofrequency catheter ablation in thirty-five patients.BMC Cardiovasc Disord. 2012 Jul 10;12:32. doi: 10.1186/1471-2261-12-32. BMC Cardiovasc Disord. 2012. PMID: 22551200 Free PMC article.
-
Common and distinctive electrocardiographic characteristics and effective catheter ablation of idiopathic ventricular arrhythmias originating from different areas of ventricular septum adjacent to atrioventricular annulus.J Cardiovasc Electrophysiol. 2018 Aug;29(8):1104-1112. doi: 10.1111/jce.13638. Epub 2018 Jun 19. J Cardiovasc Electrophysiol. 2018. PMID: 29782689
-
Electrocardiographic features, mapping and ablation of idiopathic outflow tract ventricular arrhythmias.J Interv Card Electrophysiol. 2020 Mar;57(2):207-218. doi: 10.1007/s10840-019-00617-9. Epub 2019 Oct 24. J Interv Card Electrophysiol. 2020. PMID: 31650457
-
Modern mapping and ablation techniques to treat ventricular arrhythmias from the left ventricular summit and interventricular septum.Heart Rhythm. 2020 Sep;17(9):1609-1620. doi: 10.1016/j.hrthm.2020.04.026. Epub 2020 Apr 22. Heart Rhythm. 2020. PMID: 32333973 Review.
Cited by
-
2019 HRS/EHRA/APHRS/LAHRS expert consensus statement on catheter ablation of ventricular arrhythmias.J Interv Card Electrophysiol. 2020 Oct;59(1):145-298. doi: 10.1007/s10840-019-00663-3. J Interv Card Electrophysiol. 2020. PMID: 31984466 Free PMC article.
-
The characteristics of a 12-lead electrocardiogram measuring premature ventricular contractions originating from the tricuspid annulus using the clock position method.Ann Noninvasive Electrocardiol. 2023 Mar;28(2):e13024. doi: 10.1111/anec.13024. Epub 2022 Dec 27. Ann Noninvasive Electrocardiol. 2023. PMID: 36573893 Free PMC article.
-
Radiofrequency catheter ablation of premature ventricular contractions from near the His-bundle.J Arrhythm. 2019 Feb 15;35(2):252-261. doi: 10.1002/joa3.12167. eCollection 2019 Apr. J Arrhythm. 2019. PMID: 31007790 Free PMC article.
-
Approach selection of radiofrequency catheter ablation for ventricular arrhythmias originating from the left ventricular summit: potential relevance of Pseudo Delta wave, Intrinsicoid deflection time, maximal deflection index.BMC Cardiovasc Disord. 2017 May 30;17(1):140. doi: 10.1186/s12872-017-0575-5. BMC Cardiovasc Disord. 2017. PMID: 28558750 Free PMC article.
-
Radiofrequency catheter ablation of premature ventricular contractions from the mitral annulus in patients without structural heart disease.Pacing Clin Electrophysiol. 2020 Nov;43(11):1258-1267. doi: 10.1111/pace.14063. Epub 2020 Sep 30. Pacing Clin Electrophysiol. 2020. PMID: 32901968 Free PMC article.
References
-
- Coggins DL, Lee RJ, Sweeney J, Chein WW, Van Hare G, et al. (1994) Radiofrequency catheter ablation as a cure for idiopathic tachycardia of both left and right ventricular origin. J Am Coll Cardiol 23: 1333–41. - PubMed
-
- Tsai CF, Chen SA, Tai CT, Chiang CE, Lee SH, et al. (1997) Idiopathic monomorphic ventricular tachycardia: clinical outcome, electrophysiologic characteristics and long-term results of catheter ablation. Int J Cardiol 62: 143–50. - PubMed
-
- Li YC, Lin JF, Li J, Ji KT, Lin JX. (2012) Catheter ablation of idiopathic ventricular arrhythmias originating from left ventricular epicardium adjacent to the transitional area from the great cardiac vein to the anterior interventricular vein. Int J Cardiol, doi: 10.1016/j.ijcard.2012.06.119, [Epub ahead of print]. - PubMed
-
- Ceresnak SR, Pass RH, Krumerman AK, Kim SG, Nappo L, et al. (2012) Characteristics of ventricular tachycardia arising from the inflow region of the right ventricle. J Electrocardiol 45: 385–90. - PubMed
-
- Van Herendael H, Garcia F, Lin D, Riley M, Bala R, et al. (2011) Idiopathic right ventricular arrhythmias not arising from the outflow tract: prevalence, electrocardiographic characteristics, and outcome of catheter ablation. Heart Rhythm 8: 511–8. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
