

Regional differences in islet distribution in the human pancreas--preferential beta-cell loss in the head region in patients with type 2 diabetes
- PMID: 23826303
- PMCID: PMC3691162
- DOI: 10.1371/journal.pone.0067454
Regional differences in islet distribution in the human pancreas--preferential beta-cell loss in the head region in patients with type 2 diabetes
Abstract
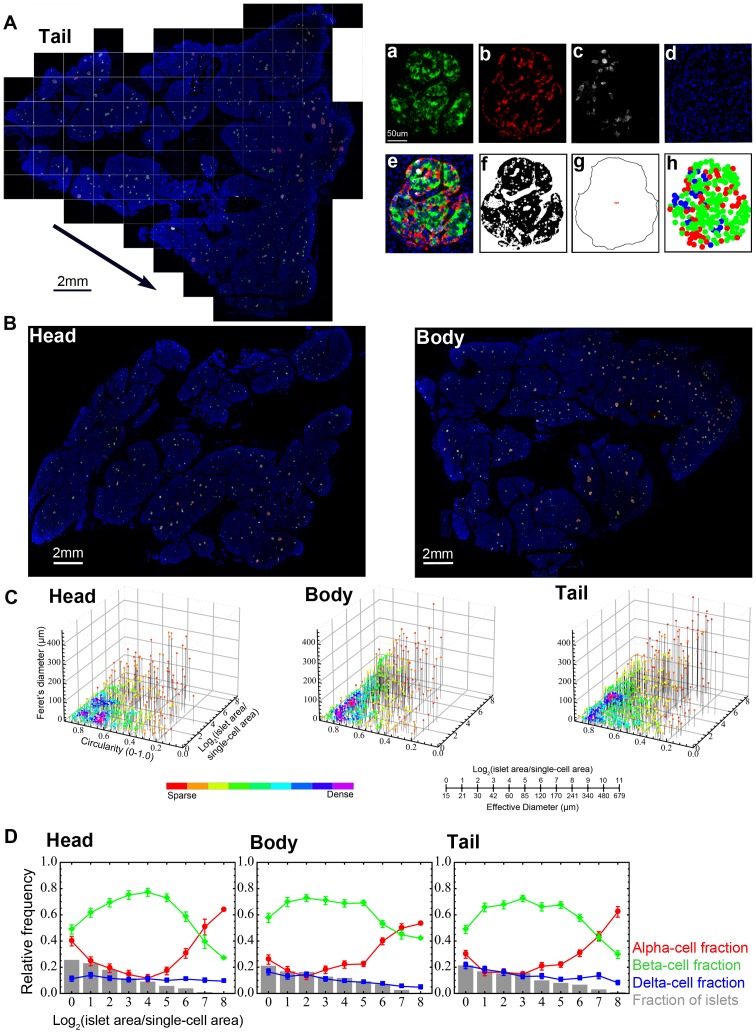
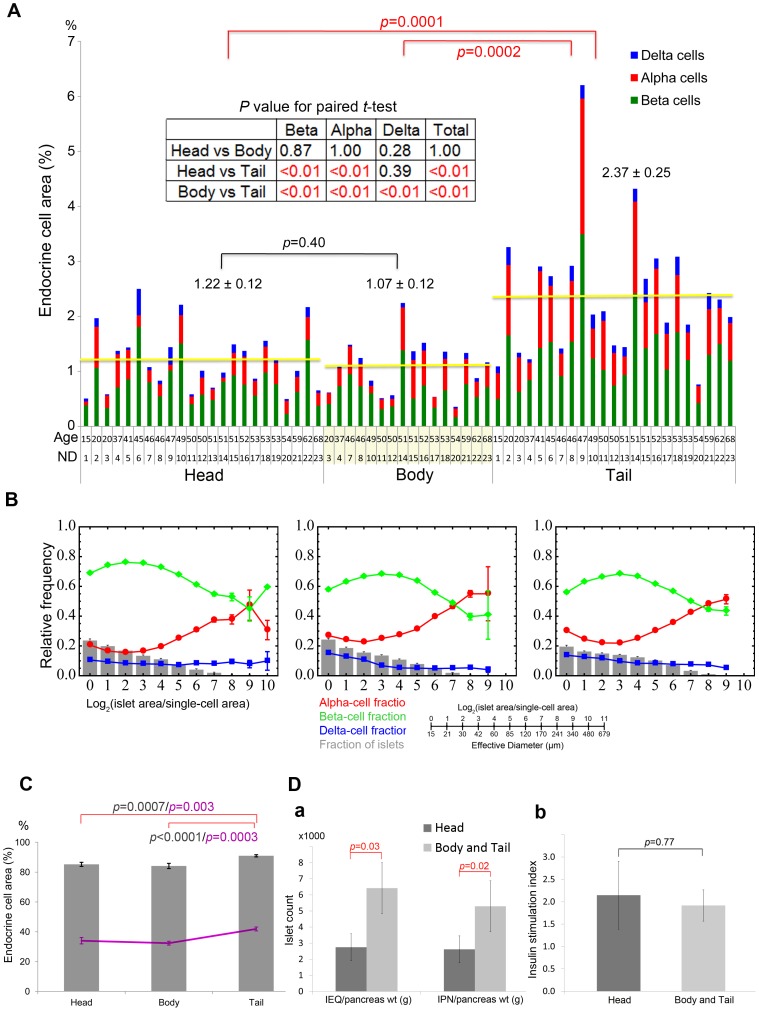
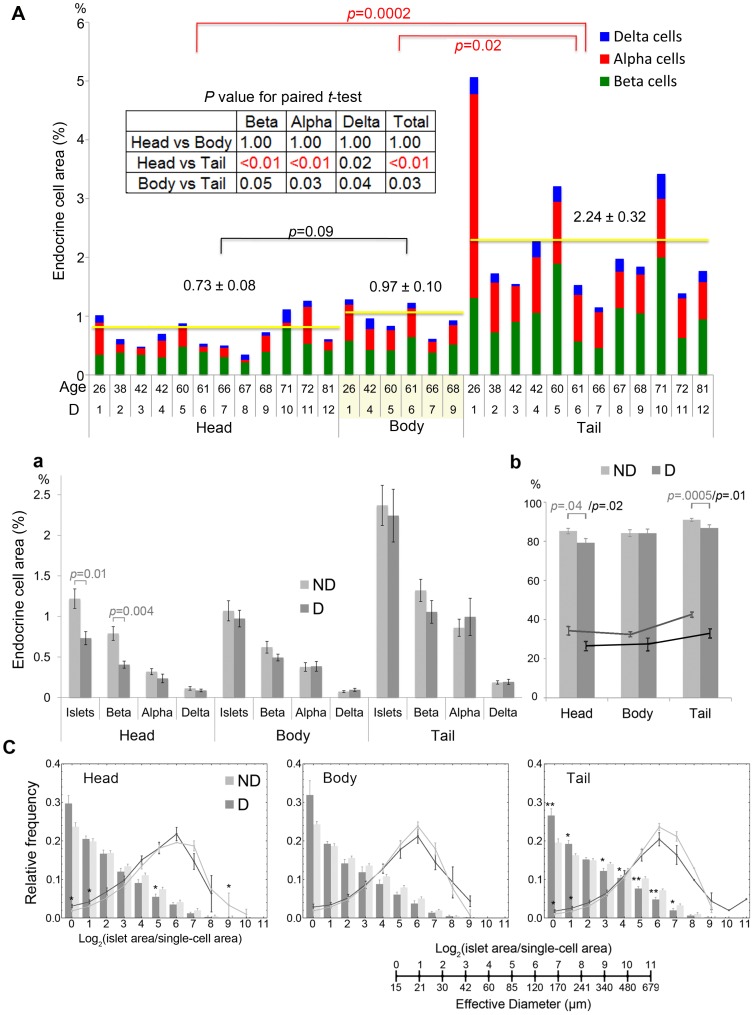
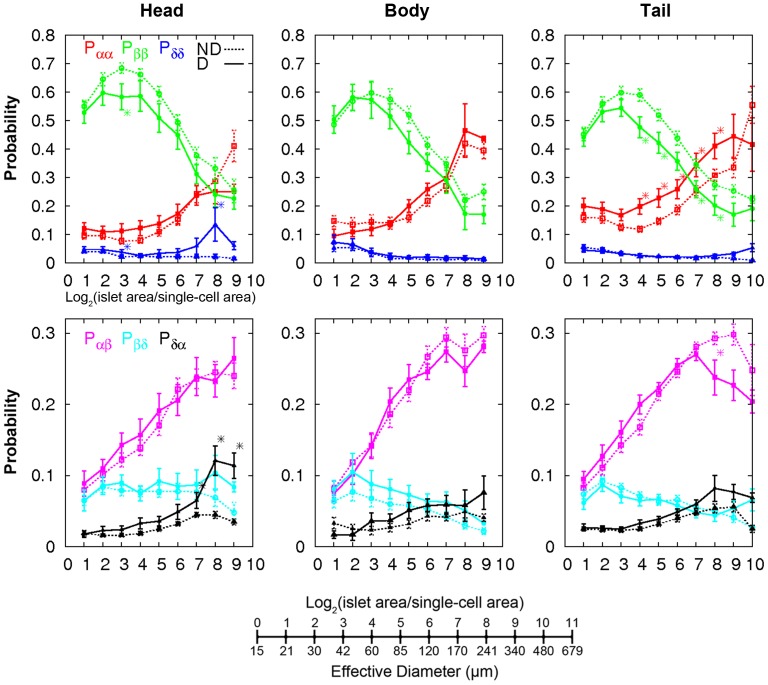
While regional heterogeneity in islet distribution has been well studied in rodents, less is known about human pancreatic histology. To fill gaps in our understanding, regional differences in the adult human pancreas were quantitatively analyzed including the pathogenesis of type 2 diabetes (T2D). Cadaveric pancreas specimens were collected from the head, body and tail regions of each donor, including subjects with no history of diabetes or pancreatic diseases (n = 23) as well as patients with T2D (n = 12). The study further included individuals from whom islets were isolated (n = 7) to study islet yield and function in a clinical setting of islet transplantation. The whole pancreatic sections were examined using an innovative large-scale image capture and unbiased detailed quantitative analyses of the characteristics of islets from each individual (architecture, size, shape and distribution). Islet distribution/density is similar between the head and body regions, but is >2-fold higher in the tail region. In contrast to rodents, islet cellular composition and architecture were similar throughout the pancreas and there was no difference in glucose-stimulated insulin secretion in islets isolated from different regions of the pancreas. Further studies revealed preferential loss of large islets in the head region in patients with T2D. The present study has demonstrated distinct characteristics of the human pancreas, which should provide a baseline for the future studies integrating existing research in the field and helping to advance bi-directional research between humans and preclinical models.
Conflict of interest statement
Figures
References
-
- Brissova M, Fowler MJ, Nicholson WE, Chu A, Hirshberg B, et al. (2005) Assessment of human pancreatic islet architecture and composition by laser scanning confocal microscopy. J Histochem Cytochem 53: 1087–1097. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
