

Pain and suicidality: insights from reward and addiction neuroscience
- PMID: 23827972
- PMCID: PMC4827340
- DOI: 10.1016/j.pneurobio.2013.06.003
Pain and suicidality: insights from reward and addiction neuroscience
Abstract
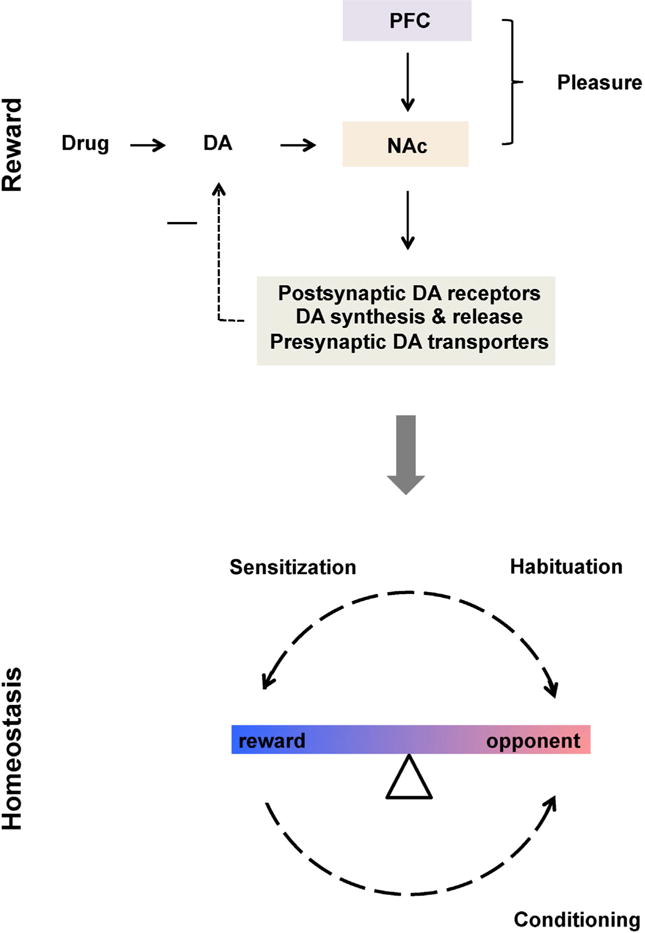
Suicidality is exceedingly prevalent in pain patients. Although the pathophysiology of this link remains unclear, it may be potentially related to the partial congruence of physical and emotional pain systems. The latter system's role in suicide is also conspicuous during setbacks and losses sustained in the context of social attachments. Here we propose a model based on the neural pathways mediating reward and anti-reward (i.e., allostatic adjustment to recurrent activation of the reward circuitry); both are relevant etiologic factors in pain, suicide and social attachments. A comprehensive literature search on neurobiology of pain and suicidality was performed. The collected articles were critically reviewed and relevant data were extracted and summarized within four key areas: (1) physical and emotional pain, (2) emotional pain and social attachments, (3) pain- and suicide-related alterations of the reward and anti-reward circuits as compared to addiction, which is the premier probe for dysfunction of these circuits and (4) mechanistically informed treatments of co-occurring pain and suicidality. Pain-, stress- and analgesic drugs-induced opponent and proponent states of the mesolimbic dopaminergic pathways may render reward and anti-reward systems vulnerable to sensitization, cross-sensitization and aberrant learning of contents and contexts associated with suicidal acts and behaviors. These findings suggest that pain patients exhibit alterations in the brain circuits mediating reward (depressed function) and anti-reward (sensitized function) that may affect their proclivity for suicide and support pain and suicidality classification among other "reward deficiency syndromes" and a new proposal for "enhanced anti-reward syndromes". We suggest that interventions aimed at restoring the balance between the reward and anti-reward networks in patients with chronic pain may help decreasing their suicide risk.
Keywords: ACC; AMY; Aberrant learning; Allostasis; Anti-reward; BLA; BNST; CEA; CRF; Cross-sensitization; DA; DBS; DMN; DRG; DSM-IV TR; Diagnostic and Statistical Manual of Mental Disorders, 4th edition, Text Revision; GABA; HB; HT; Habenula; Homeostasis; INS; LC; NAc; NE; NR; PAG; PFC; PTSD; RF; S(1); S(2); Stress; VT; amygdala; anterior cingulate gyrus; basolateral complex of the amygdala; bed nucleus the striaterminalis; central nucleus of the amygdala; corticotropin-releasing factor; deep brain stimulation; default-mode network; dopamine; dorsal root ganglion; gamma-aminobutyricacid; habenula; hypothalamus; insula; locus coeruleus; norepinephrine; nucleus accumbens; periaqueductal gray matter; posttraumatic stress disorder; prefrontal cortex; primary somatosensory cortex; raphe nuclei; reticular formation nuclei; secondary somatosensory cortex; ventral tegmentum.
Published by Elsevier Ltd.
Figures





References
-
- Ago Y, Tanaka T, Kita Y, Tokumoto H, Takuma K, Matsuda T. Lithium attenuates methamphetamine-induced hyperlocomotion and behavioral sensitization via modulation of prefrontal monoamine release. Neuropharmacology. 2012;62:1634–1639. - PubMed
-
- Alba-Delgado C, Llorca-Torralba M, Horrillo I, Ortega JE, Mico JA, Sanchez-Blazquez P, Meana JJ, Berrocoso E. Chronic pain leads to concomitant noradrenergic impairment and mood disorders. Biol Psychiatry. 2012;73:54–62. - PubMed
-
- Amat J, Sparks PD, Matus-Amat P, Griggs J, Watkins LR, Maier SF. The role of the habenular complex in the elevation of dorsal raphe nucleus serotonin and the changes in the behavioral responses produced by uncontrollable stress. Brain Res. 2001;917:118–126. - PubMed
-
- Amen DG, Prunella JR, Fallon JH, Amen B, Hanks C. A comparative analysis of completed suicide using high resolution brain SPECT imaging. J Neuropsychiatry Clin Neurosci. 2009;21:430–439. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
