

Vasoconstriction by electrical stimulation: new approach to control of non-compressible hemorrhage
- PMID: 23828130
- PMCID: PMC3701318
- DOI: 10.1038/srep02111
Vasoconstriction by electrical stimulation: new approach to control of non-compressible hemorrhage
Abstract
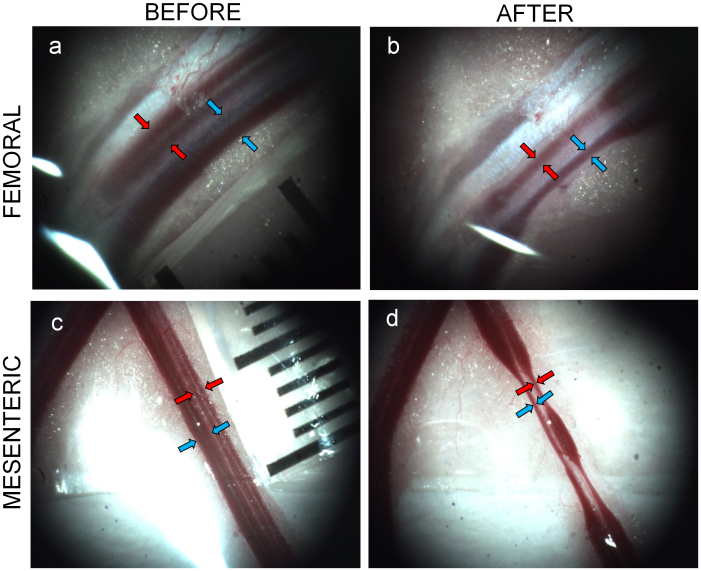
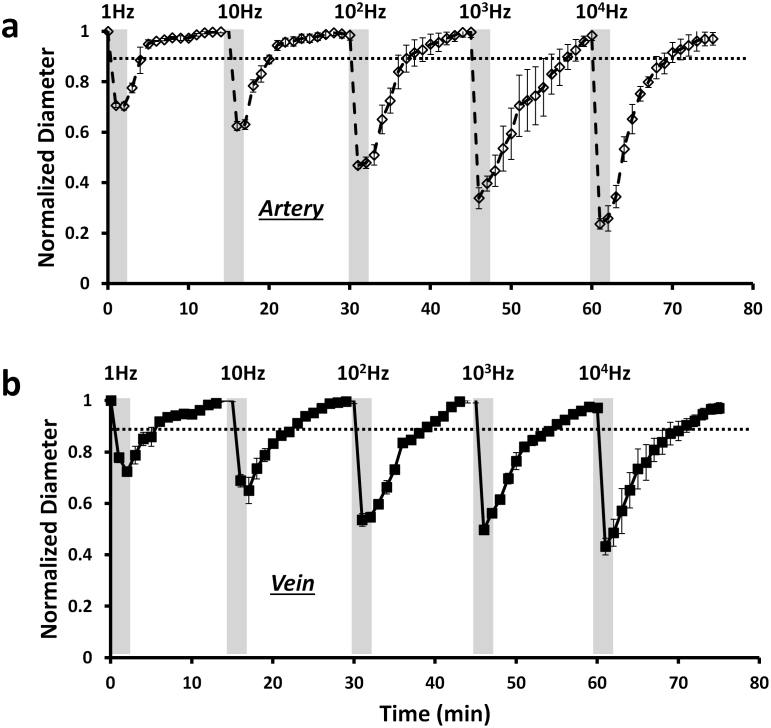
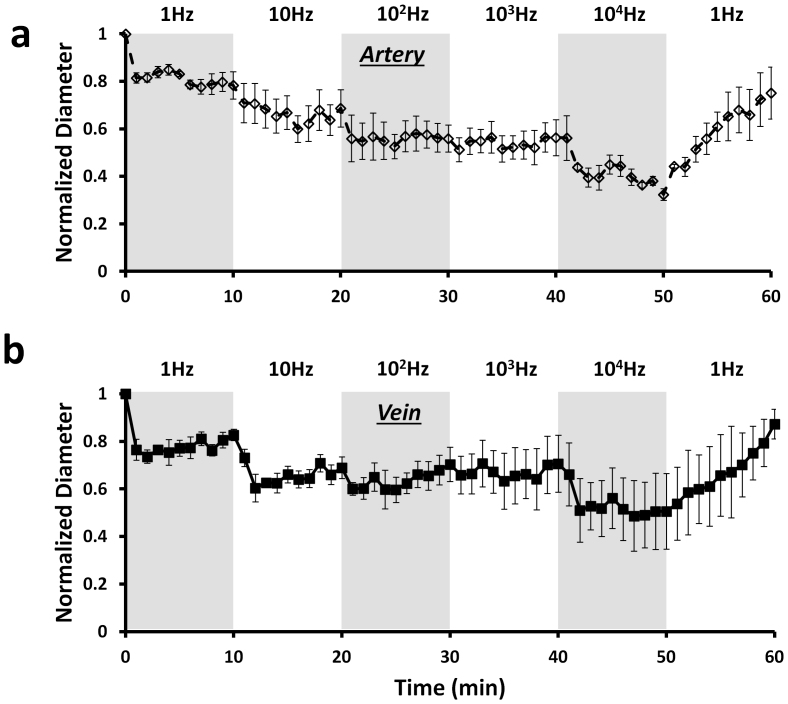
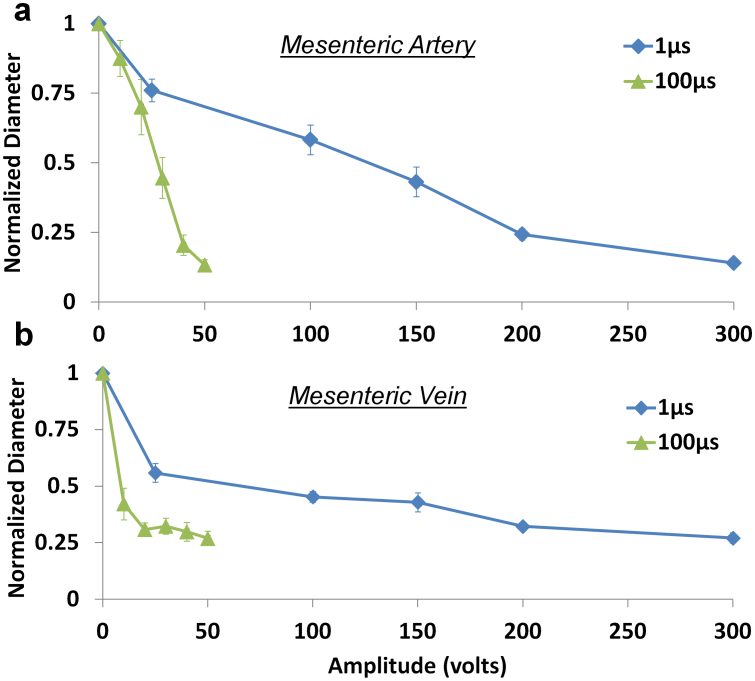
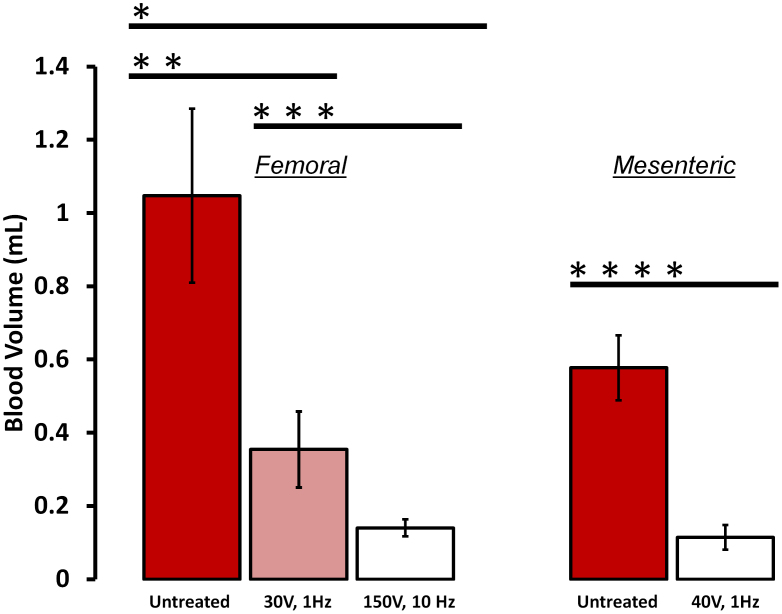
Non-compressible hemorrhage is the most common preventable cause of death on battlefield and in civilian traumatic injuries. We report the use of microsecond pulses of electric current to induce rapid constriction in femoral and mesenteric arteries and veins in rats. Electrically-induced vasoconstriction could be induced in seconds while blood vessels dilated back to their original size within minutes after stimulation. At higher settings, a blood clotting formed, leading to complete and permanent occlusion of the vessels. The latter regime dramatically decreased the bleeding rate in the injured femoral and mesenteric arteries, with a complete hemorrhage arrest achieved within seconds. The average blood loss from the treated femoral artery during the first minute after injury was about 7 times less than that of a non-treated control. This new treatment modality offers a promising approach to non-damaging control of bleeding during surgery, and to efficient hemorrhage arrest in trauma patients.
Figures



Similar articles
-
Miniature electrical stimulator for hemorrhage control.IEEE Trans Biomed Eng. 2014 Jun;61(6):1765-71. doi: 10.1109/TBME.2014.2306672. IEEE Trans Biomed Eng. 2014. PMID: 24845287
-
Mechanisms of electrical vasoconstriction.J Neuroeng Rehabil. 2018 May 29;15(1):43. doi: 10.1186/s12984-018-0390-y. J Neuroeng Rehabil. 2018. PMID: 29843762 Free PMC article.
-
Determination of efficacy of new hemostatic dressings in a model of extremity arterial hemorrhage in swine.J Trauma. 2009 Sep;67(3):450-9; discussion 459-60. doi: 10.1097/TA.0b013e3181ac0c99. J Trauma. 2009. PMID: 19741385
-
Monitoring of hemostasis in combat trauma patients.Mil Med. 2004 Dec;169(12 Suppl):11-5, 4. doi: 10.7205/milmed.169.12s.11. Mil Med. 2004. PMID: 15651434 Review.
-
Transcatheter arterial embolization in abdominal blunt trauma with active mesenteric bleeding: case series and review of literature.Emerg Radiol. 2021 Feb;28(1):55-63. doi: 10.1007/s10140-020-01831-z. Epub 2020 Jul 28. Emerg Radiol. 2021. PMID: 32725601 Review.
Cited by
-
Innervation of adipocytes is limited in mouse perivascular adipose tissue.Am J Physiol Heart Circ Physiol. 2024 Jul 1;327(1):H155-H181. doi: 10.1152/ajpheart.00041.2024. Epub 2024 May 24. Am J Physiol Heart Circ Physiol. 2024. PMID: 38787382 Free PMC article.
-
Skin rejuvenation with non-invasive pulsed electric fields.Sci Rep. 2015 May 12;5:10187. doi: 10.1038/srep10187. Sci Rep. 2015. PMID: 25965851 Free PMC article.
-
Vasospasm secondary to responsive neurostimulator placement: a previously unreported complication. Illustrative case.J Neurosurg Case Lessons. 2023 May 29;5(22):CASE22435. doi: 10.3171/CASE22435. Print 2023 May 29. J Neurosurg Case Lessons. 2023. PMID: 37249138 Free PMC article.
-
Influence of electric field, blood velocity, and pharmacokinetics on electrochemotherapy efficiency.Biophys J. 2023 Aug 22;122(16):3268-3298. doi: 10.1016/j.bpj.2023.07.004. Epub 2023 Jul 7. Biophys J. 2023. PMID: 37421133 Free PMC article.
-
In silico study about the influence of electroporation parameters on the cellular internalization, spatial uniformity, and cytotoxic effects of chemotherapeutic drugs using the Method of Fundamental Solutions.Med Biol Eng Comput. 2024 Mar;62(3):713-749. doi: 10.1007/s11517-023-02964-2. Epub 2023 Nov 21. Med Biol Eng Comput. 2024. PMID: 37989990
References
-
- Center for Disease Control (CDC): Web-based Injury Statistics Query and Reporting System (WISQARS). In: U.S. Department of Health and Human Services, CDC, National Center for Injury Prevention and Control. (2002).
-
- Kauvar D. S., Lefering R. & Wade C. E. Impact of Hemorrhage on Trauma Outcome: An Overview of Epidemiology, Clinical Presentations, and Therapeutic Considerations. J Trauma. 60(6 Suppl), S3–11 (2006). - PubMed
-
- Kragh J. F. et al. New tourniquet device concepts for battlefield hemorrhage control. US. Army Med. Dep. J. Apr–June, 38–48 (2011). - PubMed
-
- Kragh J. F. et al. Battle casualty survival with emergency tourniquet use to stop limb bleeding. J. Emerg. Med. 41(6), 590–7 (2011). - PubMed
-
- Kauvar D. S., Lefering R. & Wade C. E. Impact of hemorrhage on trauma outcome: an overview of epidemiology, clinical presentations, and therapeutic considerations. J. Trauma 60(6 Suppl), S3–11 (2006). - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
