

Pelvic heterotopic ossification: when CT comes to the aid of MR imaging
- PMID: 23828230
- PMCID: PMC3781260
- DOI: 10.1007/s13244-013-0265-5
Pelvic heterotopic ossification: when CT comes to the aid of MR imaging
Abstract
Objective: This article compares various imaging aspects of magnetic resonance (MR) and computed tomography (CT) of heterotopic ossification (HO) in the pelvic soft tissues in paraplegic patients. Our aim is to highlight the benefits of integrating MR and CT imaging in the diagnosis of immature HO, which may be challenging with MR images alone.
Methods: Paraplegic patients examined on the same day by contrast-enhanced 0.4-T pelvic MR and unenhanced CT for pressure-sore-related infections were selected. MR imaging was performed on a Hitachi-Aperto 0.4 T; the Open Magnet served as a more favourable configuration for the required limb positioning of these patients. CT images were attained on a six-slice Siemens-Somaton-Emotion.
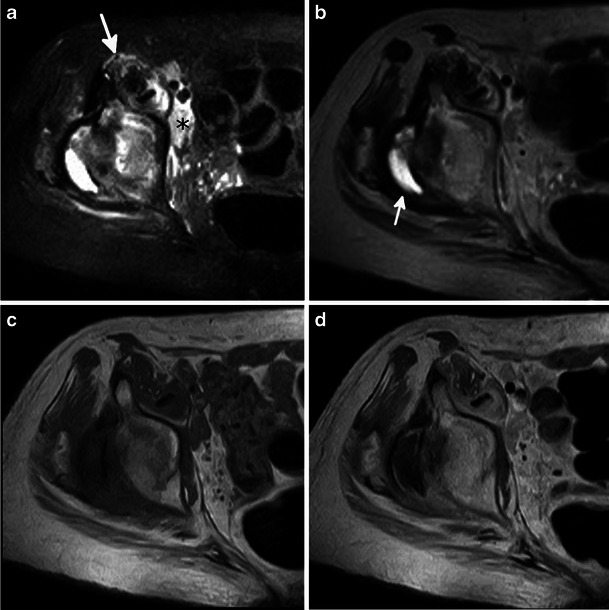
Results: MR images of HO differ according to the degree of bone maturity. The more immature the HO process, the more heterogeneous is the signal, characterised mostly by focal iso-hypointensity on T1-weighted images and hyperintensity on T2-weighted/short TI inversion recovery (STIR). These characteristics correlate to different CT patterns.
Conclusions: MR and CT features of pelvic HO in paralysed patients were reviewed with a focus on the different aspects associated with the degree of ossification. Based solely on the MR findings, immature heterotopic ossification may be difficult to differentiate from other soft tissue pelvic lesions.
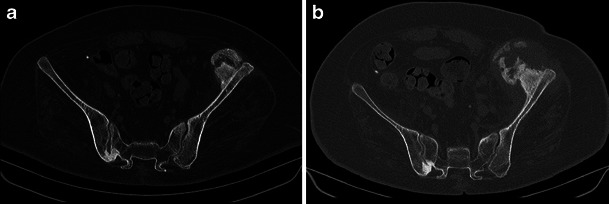
Teaching points: • The pelvis and hip are common locations of heterotopic ossifications (HO), often occurring in paraplegic patients. • With respect to HO, MR imaging allows for a confident diagnosis in mature ossified lesions only. The MR aspect of immature ossification may be confused with other pathologies. • Plain radiographs and CT may show various phases of ossification: amorphous calcification, immature and mature ossification. • Integrating MR with CT can help recognise HO foci and differentiate them from infections and other soft tissue lesions.
Figures










Similar articles
-
Pelvic heterotopic ossification: MR imaging characteristics.Radiology. 2002 Jan;222(1):189-95. doi: 10.1148/radiol.2221010552. Radiology. 2002. PMID: 11756725
-
Nasal polyps with metaplastic ossification: CT and MR imaging findings.Neuroradiology. 2010 Dec;52(12):1179-84. doi: 10.1007/s00234-010-0758-6. Epub 2010 Aug 18. Neuroradiology. 2010. PMID: 20717820
-
Pelvic MRI in spinal cord injury patients: incidence of muscle signal change and early heterotopic ossification.Spinal Cord. 2021 Jun;59(6):635-641. doi: 10.1038/s41393-020-00539-8. Epub 2020 Sep 1. Spinal Cord. 2021. PMID: 32873893
-
Heterotopic ossification in patients after total hip replacement.Ortop Traumatol Rehabil. 2007 May-Jun;9(3):264-72. Ortop Traumatol Rehabil. 2007. PMID: 17721424 Review. English, Polish.
-
Heterotopic ossification.J Nucl Med. 2002 Mar;43(3):346-53. J Nucl Med. 2002. PMID: 11884494 Review.
Cited by
-
Improving osteoarticular characterization in magnetic resonance imaging: the role of simulated computed tomography sequences.Radiol Bras. 2025 Feb 24;58:e20240048en. doi: 10.1590/0100-3984.2024.0048-en. eCollection 2025 Jan-Dec. Radiol Bras. 2025. PMID: 40061096 Free PMC article.
-
[Research progress of traumatic heterotopic ossification].Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2022 Mar 15;36(3):386-394. doi: 10.7507/1002-1892.202110078. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2022. PMID: 35293183 Free PMC article. Review. Chinese.
-
Early detection of heterotopic ossification using near-infrared optical imaging reveals dynamic turnover and progression of mineralization following Achilles tenotomy and burn injury.J Orthop Res. 2014 Nov;32(11):1416-23. doi: 10.1002/jor.22697. Epub 2014 Aug 2. J Orthop Res. 2014. PMID: 25087685 Free PMC article.
-
Excision of Intra-articular Knee Heterotopic Ossification Using a 70° Arthroscope.Case Rep Orthop. 2024 Jun 6;2024:9998388. doi: 10.1155/2024/9998388. eCollection 2024. Case Rep Orthop. 2024. PMID: 38962285 Free PMC article.
-
High Frequency Spectral Ultrasound Imaging Detects Early Heterotopic Ossification in Rodents.Stem Cells Dev. 2021 May 1;30(9):473-484. doi: 10.1089/scd.2021.0011. Epub 2021 Apr 19. Stem Cells Dev. 2021. PMID: 33715398 Free PMC article.
References
-
- Seipel R, Langner S, Platz T, et al. Neurogenic heterotopic ossification:epidemiology and morphology on conventional radiographs in an early neurological rehabilitation population. Skelet Radiol. 2011;28:151–160. - PubMed
-
- Wharton GW, Morgan TH. Heteropic ossification. J Bone Joint Surg Am. 1975;52:105–112. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
