

Toward the guidance of transbronchial biopsy: identifying pulmonary nodules with optical coherence tomography
- PMID: 23828441
- PMCID: PMC3787917
- DOI: 10.1378/chest.13-0534
Toward the guidance of transbronchial biopsy: identifying pulmonary nodules with optical coherence tomography
Erratum in
-
Correction to text in: Toward the Guidance of Transbronchial Biopsy: Identifying Pulmonary Nodules With Optical Coherence Tomography.Chest. 2019 Dec;156(6):1283. doi: 10.1016/j.chest.2019.10.010. Chest. 2019. PMID: 31812207 Free PMC article. No abstract available.
Abstract
Background: Solitary pulmonary nodules (SPNs) frequently require transbronchial needle aspiration (TBNA) or biopsy to determine malignant potential, but have variable diagnostic yields. Confirming needle placement within SPNs during TBNA could significantly increase diagnostic yield. Optical coherence tomography (OCT) provides nondestructive, high-resolution, microstructural imaging with potential to distinguish SPN from parenchyma. We have developed needle-based OCT probes compatible with TBNA. Before OCT can play any significant role in guiding clinical TBNA, OCT interpretation criteria for differentiating SPN from lung parenchyma must be developed and validated.
Methods: OCT of SPN and parenchyma was performed on 111 ex vivo resection specimens. OCT criteria for parenchyma and SPN were developed and validated in a blinded assessment. Six blinded readers (two pulmonologists, two pathologists, and two OCT experts) were trained on imaging criteria in a 15-min training session prior to interpreting the validation data set.
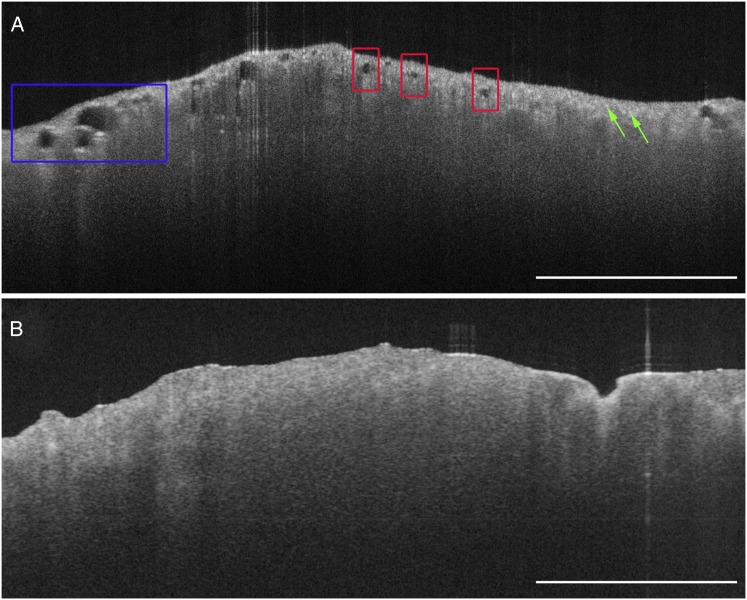
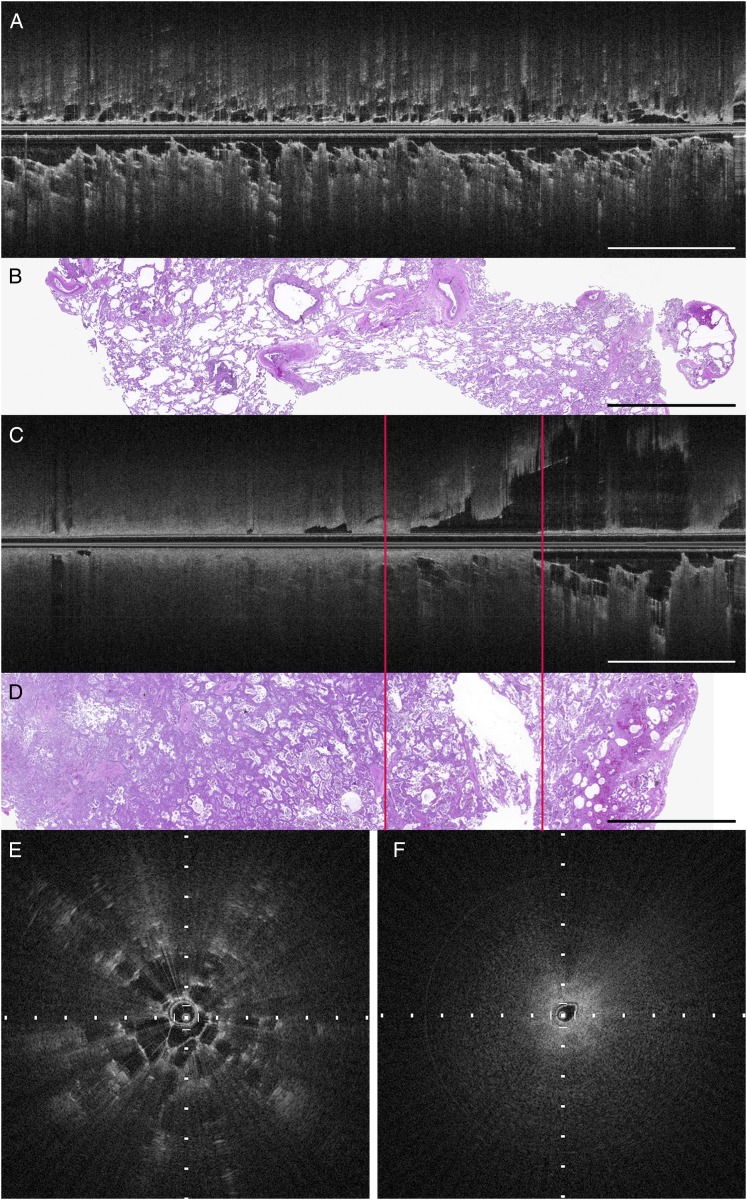
Results: OCT of lung parenchyma displayed evenly spaced signal-void alveolar spaces, signal-intense backreflections at tissue-air interfaces, or both. SPNs lacked both of these imaging features. Independent validation of OCT criteria by the six blinded readers demonstrated sensitivity and specificity of 95.4% and 98.2%, respectively.
Conclusions: We have developed and validated OCT criteria for lung parenchyma and SPN with sensitivity and specificity > 95% in this ex vivo study. We anticipate that OCT could be a useful complementary imaging modality to confirm needle placement during TBNA to potentially increase diagnostic yield.
Figures
References
-
- Gould MK, Fletcher J, Iannettoni MD, et al. Evaluation of patients with pulmonary nodules: when is it lung cancer? ACCP evidence-based clinical practice guidelines (2nd ed). Chest. 2007;132(suppl 3):108S-130S - PubMed
-
- Baaklini WA, Reinoso MA, Gorin AB, Sharafkaneh A, Manian P. Diagnostic yield of fiberoptic bronchoscopy in evaluating solitary pulmonary nodules. Chest. 2000;117(4):1049-1054 - PubMed
-
- Rivera MP, Mehta AC. Initial diagnosis of lung cancer: ACCP evidence-based clinical practice guidelines (2nd edition). Chest. 2007;132(suppl 3):131S-148S - PubMed
-
- Mazzone P, Jain P, Arroliga AC, Matthay RA. Bronchoscopy and needle biopsy techniques for diagnosis and staging of lung cancer. Clin Chest Med. 2002;23(1):137-158 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
