

An economic model to evaluate cost-effectiveness of computer assisted knee replacement surgery in Norway
- PMID: 23829478
- PMCID: PMC3722089
- DOI: 10.1186/1471-2474-14-202
An economic model to evaluate cost-effectiveness of computer assisted knee replacement surgery in Norway
Abstract
Background: The use of Computer Assisted Surgery (CAS) for knee replacements is intended to improve the alignment of knee prostheses in order to reduce the number of revision operations. Is the cost effectiveness of computer assisted surgery influenced by patient volume and age?
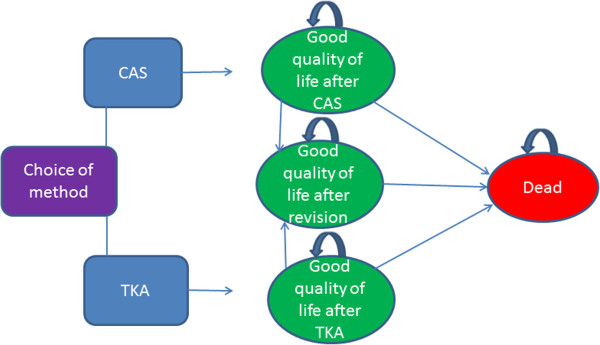
Methods: By employing a Markov model, we analysed the cost effectiveness of computer assisted surgery versus conventional arthroplasty with respect to implant survival and operation volume in two theoretical Norwegian age cohorts. We obtained mortality and hospital cost data over a 20-year period from Norwegian registers. We presumed that the cost of an intervention would need to be below NOK 500,000 per QALY (Quality Adjusted Life Year) gained, to be considered cost effective.
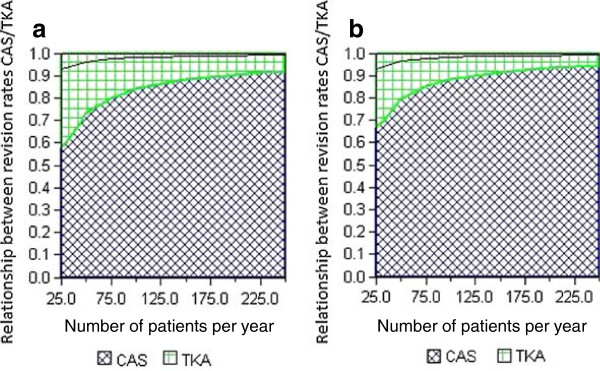
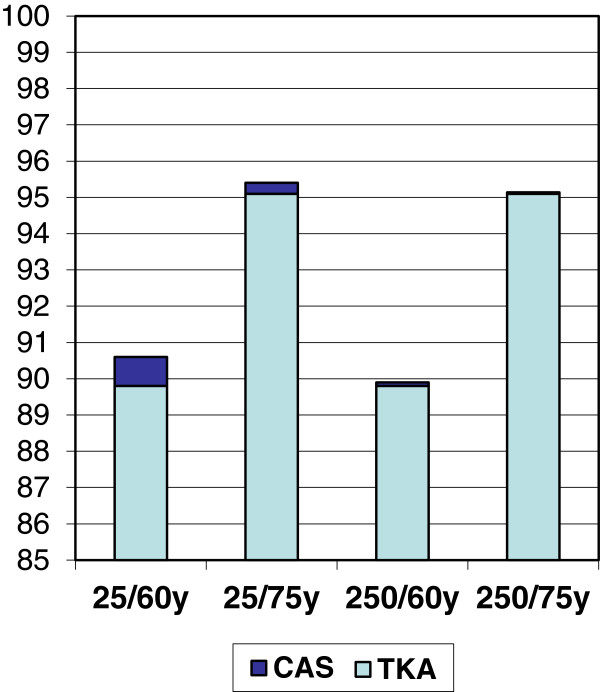
Results: The added cost of computer assisted surgery, provided this has no impact on implant survival, is NOK 1037 and NOK 1414 respectively for 60 and 75-year-olds per quality-adjusted life year at a volume of 25 prostheses per year, and NOK 128 and NOK 175 respectively at a volume of 250 prostheses per year. Sensitivity analyses showed that the 10-year implant survival in cohort 1 needs to rise from 89.8% to 90.6% at 25 prostheses per year, and from 89.8 to 89.9% at 250 prostheses per year for computer assisted surgery to be considered cost effective. In cohort 2, the required improvement is a rise from 95.1% to 95.4% at 25 prostheses per year, and from 95.10% to 95.14% at 250 prostheses per year.
Conclusions: The cost of using computer navigation for total knee replacements may be acceptable for 60-year-old as well as 75-year-old patients if the technique increases the implant survival rate just marginally, and the department has a high operation volume. A low volume department might not achieve cost-effectiveness unless computer navigation has a more significant impact on implant survival, thus may defer the investments until such data are available.
Figures

Similar articles
-
Impact of hospital volume on the economic value of computer navigation for total knee replacement.J Bone Joint Surg Am. 2008 Jul;90(7):1492-500. doi: 10.2106/JBJS.G.00888. J Bone Joint Surg Am. 2008. PMID: 18594098 Free PMC article.
-
The cost-effectiveness of computer-assisted navigation in total knee arthroplasty.J Bone Joint Surg Am. 2007 Nov;89(11):2389-97. doi: 10.2106/JBJS.F.01109. J Bone Joint Surg Am. 2007. PMID: 17974880
-
Threshold for Computer- and Robot-Assisted Knee and Hip Replacements in the English National Health Service.Value Health. 2020 Jun;23(6):719-726. doi: 10.1016/j.jval.2019.11.011. Epub 2020 May 25. Value Health. 2020. PMID: 32540229
-
Navigation knee replacement.Int Orthop. 2009 Feb;33(1):7-10. doi: 10.1007/s00264-008-0671-3. Epub 2008 Oct 29. Int Orthop. 2009. PMID: 18958468 Free PMC article. Review.
-
Computer-assisted navigation in knee arthroplasty: a critical appraisal.J Knee Surg. 2013 Oct;26(5):357-61. doi: 10.1055/s-0033-1341581. Epub 2013 Mar 19. J Knee Surg. 2013. PMID: 23512544 Review.
Cited by
-
A Systematic Literature Review of Three Modalities in Technologically Assisted TKA.Adv Orthop. 2015;2015:719091. doi: 10.1155/2015/719091. Epub 2015 Nov 18. Adv Orthop. 2015. PMID: 26664755 Free PMC article. Review.
-
How are we addressing ligament balance in TKA? A literature review of revision etiology and technological advancement.J Clin Orthop Trauma. 2016 Oct-Dec;7(4):248-255. doi: 10.1016/j.jcot.2016.04.001. Epub 2016 Aug 3. J Clin Orthop Trauma. 2016. PMID: 27857498 Free PMC article.
-
The current state of robotics in total knee arthroplasty.EFORT Open Rev. 2021 Apr 1;6(4):270-279. doi: 10.1302/2058-5241.6.200052. eCollection 2021 Apr. EFORT Open Rev. 2021. PMID: 34040804 Free PMC article. Review.
-
A systematic review on the cost-effectiveness of the computer-assisted orthopedic system.Health Care Sci. 2022 Nov 2;1(3):173-185. doi: 10.1002/hcs2.23. eCollection 2022 Dec. Health Care Sci. 2022. PMID: 38938554 Free PMC article. Review.
-
A Study of Surgical Accuracy with X-Ray-Based Patient-Specific Instrument (X3DPSI®) vs Conventional Instrument in Total Knee Arthroplasty Surgeries.Indian J Orthop. 2022 Apr 5;56(7):1240-1250. doi: 10.1007/s43465-022-00623-6. eCollection 2022 Jul. Indian J Orthop. 2022. PMID: 35813546 Free PMC article.
References
-
- Ethgen O, Bruyere O, Richy F, Dardennes C, Reginster JY. Health-related quality of life in total hip and total knee arthroplasty. A qualitative and systematic review of the literature. J Bone Joint Surg Am. 2004;86-A(5):963–974. - PubMed
-
- Saleh KJ, Celebrezze M, Kassim R, Dykes DC, Gioe TJ, Callaghan JJ. et al.Functional outcome after revision hip arthroplasty: a metaanalysis. Clin Orthop Relat Res. 2003;416:254–264. - PubMed
-
- Furnes O, Havelin LI, Espehaug B, Steindal K, Soeraas TE. The Norwegian arthroplasty register. Annual report 2009. 2009. p. 62.
-
- Jeffery RS, Morris RW, Denham RA. Coronal alignment after total knee replacement. J Bone Joint Surg Br. 1991;73(5):709–714. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
