

Parastomal hernias successfully repaired using a modified components separation method: two case reports
- PMID: 23830070
- PMCID: PMC3711726
- DOI: 10.1186/1752-1947-7-180
Parastomal hernias successfully repaired using a modified components separation method: two case reports
Abstract
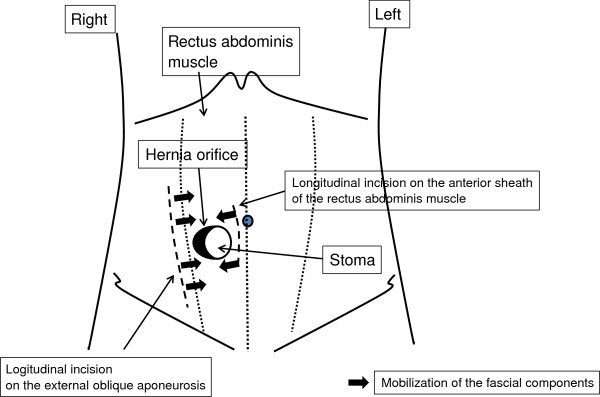
Introduction: Parastomal hernia is a frequent complication after enterostomy formation. A repair using prosthetic mesh by way of a laparoscopic or open transabdominal approach is usually recommended, however, other procedures may be done if the repair is to be performed in a contaminated environment or when the abdominal cavity of the patient is difficult to enter due to postsurgical dense adhesion. The components separation method, which was introduced for non-transabdominal and non-prosthetic ventral hernia repair, solves such problems.
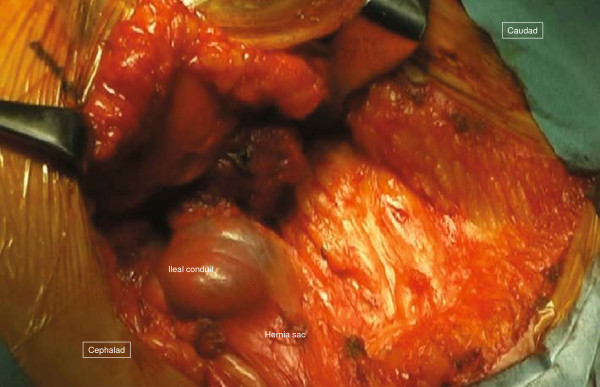
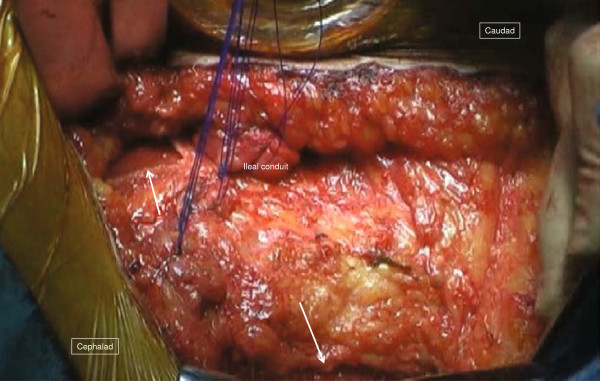
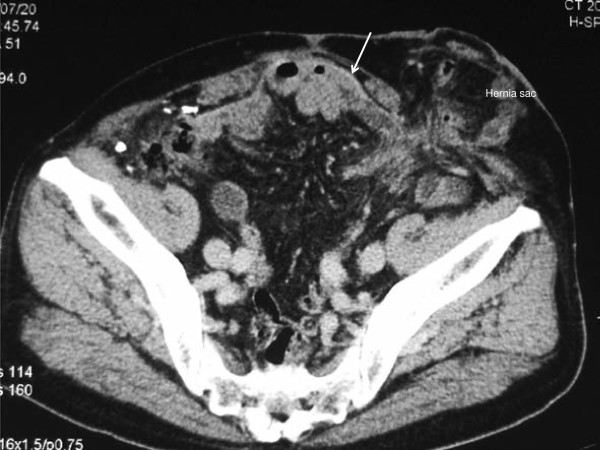
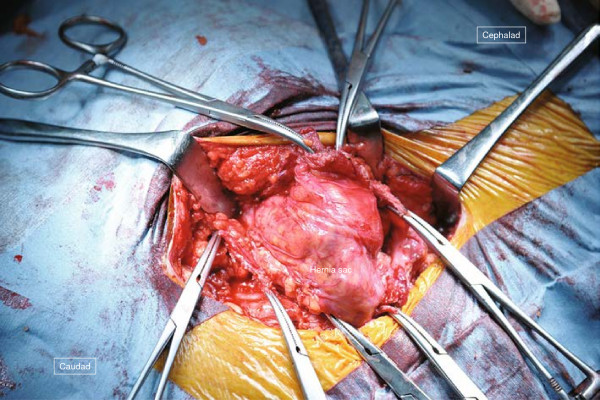
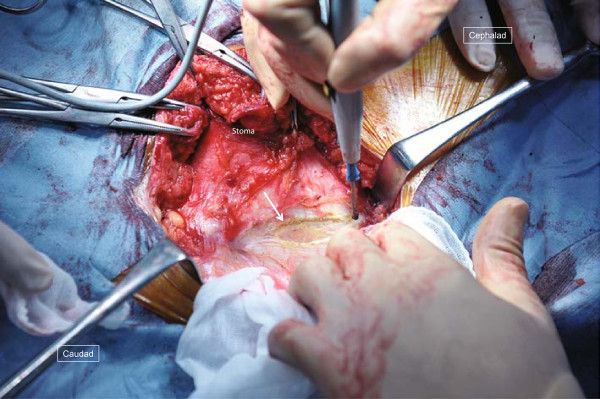
Case presentation: Case 1. A 79-year-old Japanese woman who underwent total cystectomy with ileal conduit for bladder cancer presented with a parastomal hernia, which was repaired using a keyhole technique. Simultaneously, an incisional hernia in the midline was repaired with a prosthetic mesh. One year after her hernia surgery, a recurrence occurred lateral to the stoma, but it was believed to be difficult to enter the peritoneal cavity because of the wide placement of mesh. Therefore, surgery using the components separation method was performed.
Conclusion: The components separation method is a novel and effective technique for parastomal hernia repair, especially in cases following abdominal polysurgery or midline incisional hernia repairs using large pieces of mesh. To the best of our knowledge, this is the first report in English on the application of the components separation method for parastomal hernia repair.
Figures


Similar articles
-
Robotic retro-rectus repair of parastomal hernias.J Robot Surg. 2019 Jun;13(3):483-489. doi: 10.1007/s11701-018-0874-6. Epub 2018 Sep 24. J Robot Surg. 2019. PMID: 30251135
-
Laparoscopic repair for recurrent parastomal hernia of an end stoma using the sandwich technique while preserving an ileal conduit: A case report.Int J Surg Case Rep. 2016;25:75-8. doi: 10.1016/j.ijscr.2016.06.007. Epub 2016 Jun 16. Int J Surg Case Rep. 2016. PMID: 27337702 Free PMC article.
-
Case Report: Combined Laparoscopic Perineal Hernia and Abdominal Parastomal Hernia Repair With a Mesh After Abdominoperineal Resection: A Video Vignette and Review of the Literature.J Abdom Wall Surg. 2024 Nov 22;3:13261. doi: 10.3389/jaws.2024.13261. eCollection 2024. J Abdom Wall Surg. 2024. PMID: 39651457 Free PMC article.
-
[Parastomal hernia treatment with prosthetic mesh repair].Chirurg. 2010 Mar;81(3):216-21. doi: 10.1007/s00104-009-1820-y. Chirurg. 2010. PMID: 20238203 Review. German.
-
Parastomal hernia: complications of extra-peritoneal onlay mesh placement.Hernia. 2009 Oct;13(5):487-90. doi: 10.1007/s10029-009-0494-1. Epub 2009 Mar 26. Hernia. 2009. PMID: 19322626 Review.
Cited by
-
Laparoscopic modified Sugarbaker parastomal hernia repair with 2-point anchoring and zigzag tacking of Parietex™ Parastomal Mesh technique.Surg Endosc. 2016 Dec;30(12):5628-5634. doi: 10.1007/s00464-016-4927-5. Epub 2016 Apr 29. Surg Endosc. 2016. PMID: 27129541
References
-
- Riansuwan W, Hull TL, Millan MM, Hammel JP. Surgery of recurrent parastomal hernia: direct repair or relocation? Colorectal Dis. 2010;12:681–686. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
