

Optical coherence tomography-based observation of the natural history of drusenoid lesion in eyes with dry age-related macular degeneration
- PMID: 23830761
- PMCID: PMC5340146
- DOI: 10.1016/j.ophtha.2013.05.029
Optical coherence tomography-based observation of the natural history of drusenoid lesion in eyes with dry age-related macular degeneration
Abstract
Purpose: To use spectral domain optical coherence tomography (SD-OCT) to investigate risk factors predictive for the development of atrophy of drusenoid lesions (DLs) (drusen and drusenoid pigment epithelium detachment) in eyes with non-neovascular age-related macular degeneration (NNVAMD).
Design: Cohort study.
Participants: Forty-one eyes from 29 patients with NNVAMD.
Methods: Patients with NNVAMD who underwent registered SD-OCT imaging over a minimum period of 6 months were reviewed. Drusenoid lesions that were accompanied by new atrophy onset at 6 months or last follow-up (FUL) were further analyzed. Detailed lesion change was described throughout the study period. Odds ratios (ORs) and risk for new local atrophy onset were calculated.
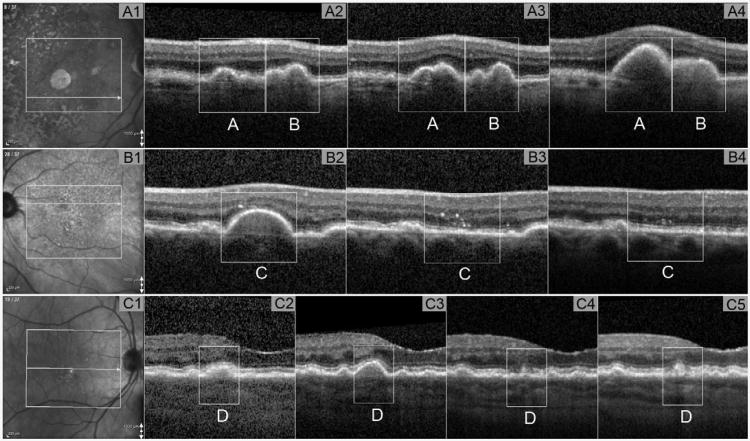
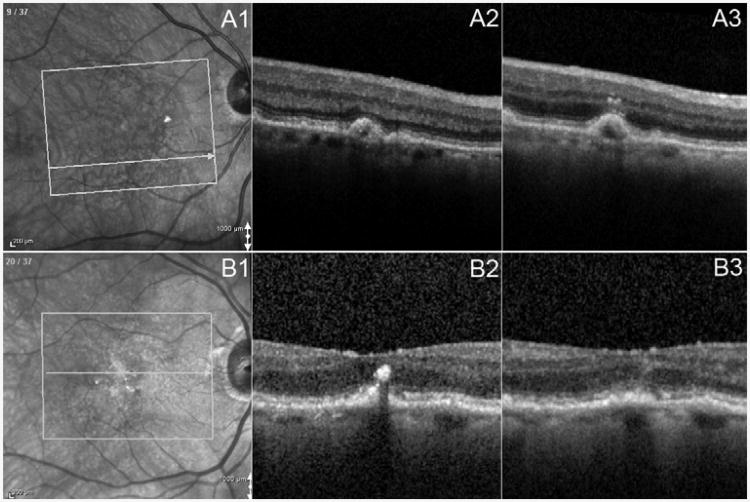
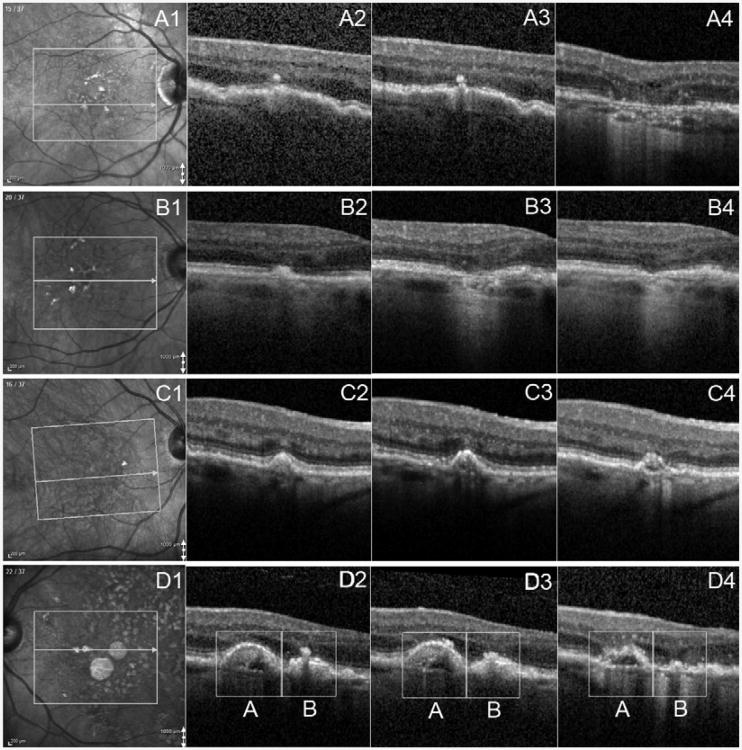
Main outcome measures: Drusenoid lesion features and longitudinal changes in features, including maximum lesion height, lesion diameter, lesion internal reflectivity, and presence and extent of overlying intraretinal hyperreflective foci (HRF). Subfoveal choroidal thickness (SFCT) and choroidal thickness (CT) were measured below each lesion.
Results: A total of 543 individual DLs were identified at baseline, and 28 lesions developed during follow-up. The mean follow-up time was 21.3±8.6 months (range, 6-44 months). Some 3.2% of DLs (18/571) progressed to atrophy within 18.3 ± 9.5 months (range, 5-28 months) of the initial visit. Drusenoid lesions with heterogeneous internal reflectivity were significantly associated with new atrophy onset at 6 months (OR, 5.614; 95% confidence interval [CI], 1.277-24.673) and new atrophy onset at FUL (OR, 7.005; 95% CI, 2.300-21.337). Lesions with the presence of HRF were significant predictors of new atrophy onset at 6 months (OR, 30.161; 95% CI, 4.766-190.860) and FUL (OR, 11.211; 95% CI, 2.513-50.019). Lesions with a baseline maximum height >80 μm or CT ≤ 135 μm showed a positive association with the new atrophy onset at FUL (OR, 7.886; 95% CI, 2.105-29.538 and OR, 3.796; 95% CI, 1.154-12.481, respectively).
Conclusions: The presence of HRF overlying DLs, a heterogeneous internal reflectivity of these lesions, was found consistently to be predictive of local atrophy onset in the ensuing months. These findings provide further insight into the natural history of anatomic change occurring in patients with NNVAMD.
Copyright © 2013 American Academy of Ophthalmology. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Bird AC, Marshall J. Retinal pigment epithelial detachments in the elderly. Transactions of the ophthalmological societies of the United Kingdom. 1986;105(6):674–82. - PubMed
-
- Zweifel SA, Imamura Y, Spaide TC, et al. Prevalence and significance of subretinal drusenoid deposits (reticular pseudodrusen) in age-related macular degeneration. Ophthalmology. 2010;117:1775–81. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
