

Current management of calcific aortic stenosis
- PMID: 23833296
- PMCID: PMC4013234
- DOI: 10.1161/CIRCRESAHA.111.300084
Current management of calcific aortic stenosis
Abstract
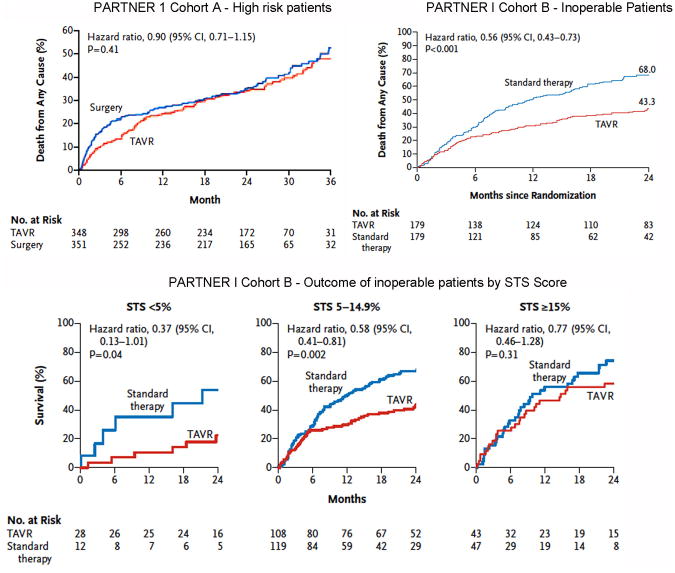
Calcific aortic stenosis is a progressive disease with no effective medical therapy that ultimately requires aortic valve replacement (AVR) for severe valve obstruction. Echocardiography is the primary diagnostic approach to define valve anatomy, measure aortic stenosis severity, and evaluate the left ventricular response to chronic pressure overload. In asymptomatic patients, markers of disease progression include the degree of leaflet calcification, hemodynamic severity of stenosis, adverse left ventricular remodeling, reduced left ventricular longitudinal strain, myocardial fibrosis, and pulmonary hypertension. The onset of symptoms portends a predictably high mortality rate unless AVR is performed. In symptomatic patients, AVR improves symptoms, improves survival, and, in patients with left ventricular dysfunction, improves systolic function. Poor outcomes after AVR are associated with low-flow low-gradient aortic stenosis, severe ventricular fibrosis, oxygen-dependent lung disease, frailty, advanced renal dysfunction, and a high comorbidity score. However, in most patients with severe symptoms, AVR is lifesaving. Bioprosthetic valves are recommended for patients aged >65 years. Transcatheter AVR is now available for patients with severe comorbidities, is recommended in patients who are deemed inoperable, and is a reasonable alternative to surgical AVR in high-risk patients.
Keywords: aortic valve stenosis; heart failure; heart valve diseases; heart valve prosthesis; hypertrophy, left ventricular.
Figures

References
-
- Stewart BF, Siscovick D, Lind BK, Gardin JM, Gottdiener JS, Smith VE, Kitzman DW, Otto CM. Clinical factors associated with calcific aortic valve disease. Cardiovascular Health Study. J Am Coll Cardiol. 1997;29:630–634. - PubMed
-
- Otto CM, Lind BK, Kitzman DW, Gersh BJ, Siscovick DS. Association of aortic-valve sclerosis with cardiovascular mortality and morbidity in the elderly. N Engl J Med. 1999;341:142–147. - PubMed
-
- Nkomo VT, Gardin JM, Skelton TN, Gottdiener JS, Scott CG, Enriquez-Sarano M. Burden of valvular heart diseases: a population-based study. Lancet. 2006;368:1005–1011. - PubMed
-
- Novaro GM, Katz R, Aviles RJ, Gottdiener JS, Cushman M, Psaty BM, Otto CM, Griffin BP. Clinical factors, but not C-reactive protein, predict progression of calcific aortic-valve disease: the Cardiovascular Health Study. J Am Coll Cardiol. 2007;50:1992–1998. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
