

AKI in hospitalized children: epidemiology and clinical associations in a national cohort
- PMID: 23833312
- PMCID: PMC3789331
- DOI: 10.2215/CJN.00270113
AKI in hospitalized children: epidemiology and clinical associations in a national cohort
Abstract
Background and objectives: Although AKI is common among hospitalized children, comprehensive epidemiologic data are lacking. This study characterizes pediatric AKI across the United States and identifies AKI risk factors using high-content/high-throughput analytic techniques.
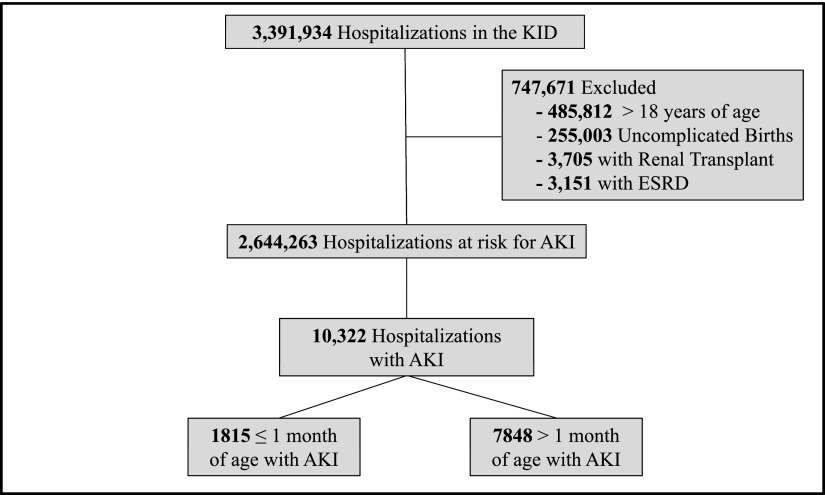
Design, setting, participants, & measurements: For the cross-sectional analysis of the 2009 Kids Inpatient Database, AKI events were identified using International Classification of Diseases, Ninth Revision, Clinical Modification codes. Demographics, incident rates, and outcome data were analyzed and reported for the entire AKI cohort as well as AKI subsets. Statistical learning methods were applied to the highly imbalanced dataset to derive AKI-related risk factors.
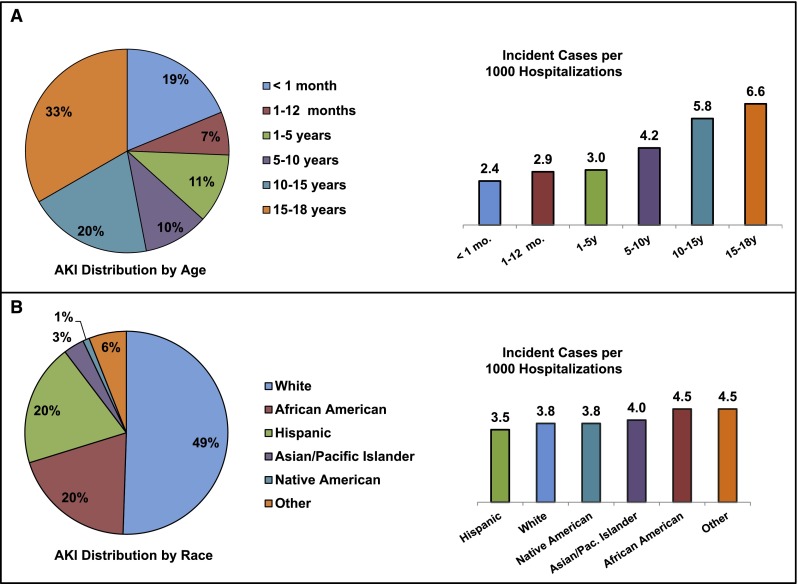
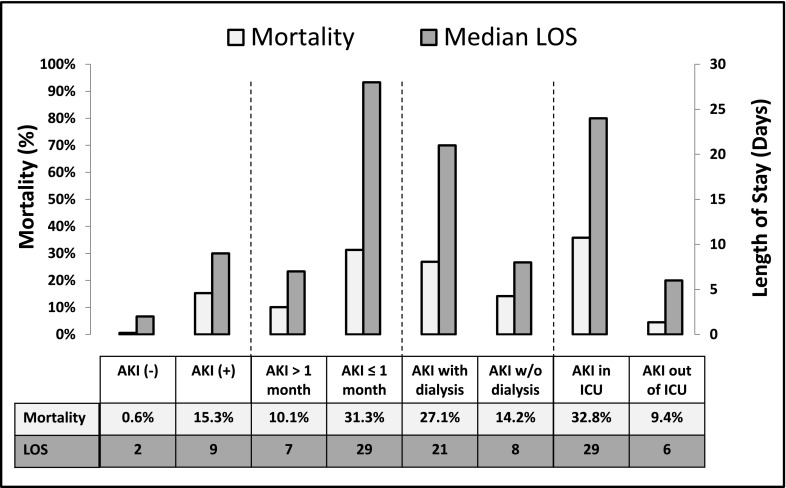
Results: Of 2,644,263 children, 10,322 children developed AKI (3.9/1000 admissions). Although 19% of the AKI cohort was ≤ 1 month old, the highest incidence was seen in children 15-18 years old (6.6/1000 admissions); 49% of the AKI cohort was white, but AKI incidence was higher among African Americans (4.5 versus 3.8/1000 admissions). In-hospital mortality among patients with AKI was 15.3% but higher among children ≤ 1 month old (31.3% versus 10.1%, P<0.001) and children requiring critical care (32.8% versus 9.4%, P<0.001) or dialysis (27.1% versus 14.2%, P<0.001). Shock (odds ratio, 2.15; 95% confidence interval, 1.95 to 2.36), septicemia (odds ratio, 1.37; 95% confidence interval, 1.32 to 1.43), intubation/mechanical ventilation (odds ratio, 1.2; 95% confidence interval, 1.16 to 1.25), circulatory disease (odds ratio, 1.47; 95% confidence interval, 1.32 to 1.65), cardiac congenital anomalies (odds ratio, 1.2; 95% confidence interval, 1.13 to 1.23), and extracorporeal support (odds ratio, 2.58; 95% confidence interval, 2.04 to 3.26) were associated with AKI.
Conclusions: AKI occurs in 3.9/1000 at-risk US pediatric hospitalizations. Mortality is highest among neonates and children requiring critical care or dialysis. Identified risk factors suggest that AKI occurs in association with systemic/multiorgan disease more commonly than primary renal disease.
Figures
References
-
- Xue JL, Daniels F, Star RA, Kimmel PL, Eggers PW, Molitoris BA, Himmelfarb J, Collins AJ: Incidence and mortality of acute renal failure in Medicare beneficiaries, 1992 to 2001. J Am Soc Nephrol 17: 1135–1142, 2006 - PubMed
-
- Vachvanichsanong P, Dissaneewate P, Lim A, McNeil E: Childhood acute renal failure: 22-year experience in a university hospital in southern Thailand. Pediatrics 118: e786–e791, 2006 - PubMed
-
- Chertow GM, Burdick E, Honour M, Bonventre JV, Bates DW: Acute kidney injury, mortality, length of stay, and costs in hospitalized patients. J Am Soc Nephrol 16: 3365–3370, 2005 - PubMed
-
- Alkandari O, Eddington KA, Hyder A, Gauvin F, Ducruet T, Gottesman R, Phan V, Zappitelli M: Acute kidney injury is an independent risk factor for pediatric intensive care unit mortality, longer length of stay and prolonged mechanical ventilation in critically ill children: A two-center retrospective cohort study. Crit Care 15: R146, 2011 - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
