

doi: 10.4103/0971-3026.111481.
Shoulder ultrasound: What you need to know
Affiliations
- PMID: 23833420
- PMCID: PMC3698891
- DOI: 10.4103/0971-3026.111481
Item in Clipboard
Shoulder ultrasound: What you need to know
Indian J Radiol Imaging.
2012 Oct.
Abstract
Shoulder ultrasound is consistently used in the assessment of rotator cuff and is as accurate as magnetic resonance imaging in the detection of rotator cuff tear. It can be used as a focused examination providing rapid, real-time diagnosis, and treatment in desired clinical situations. This article presents a simplified approach to scanning and image-guided intervention, and discusses common sonographically apparent shoulder pathologies.
Keywords: Shoulder; pathology; technique; ultrasound.
Conflict of interest statement
Figures
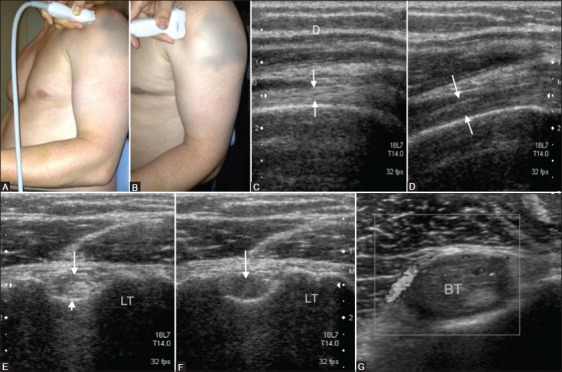
(A-G): Biceps tendon. Probe placement to examine long head of the biceps tendon in transverse plane (A) and longitudinal plane (B). Long head of biceps tendon (arrows) in longitudinal (C) and transverse plane (E) appears hypoechoic (D and F) (arrows) due to anisotrophy when not imaged perpendicular to the sound beam. Hypoechoic appearance (G) of biceps tendon with areas of increased Doppler signal as a result of tendinopathy. LT: Lesser tuberosity
(A, B): (A) Transverse scan of torn long head of biceps tendon with an empty bicipital groove (arrow). (B) Longitudinal scan shows the convex superior margin (arrow) of the retracted muscle belly (popeye sign). LT: Lesser tuberosity, D: Deltoid
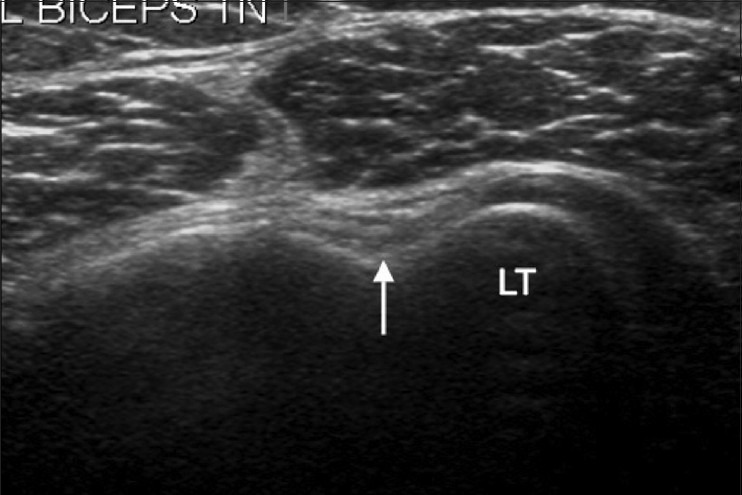
Short-axis view of the long head of the biceps tendon with bicipital groove (arrow) filled with scar tissue simulating an attenuated biceps tendon. LT: Lesser tuberosity
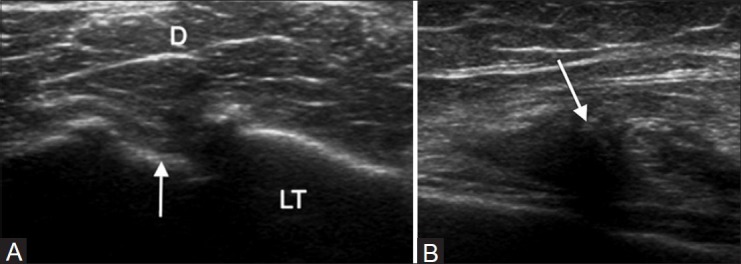
(A, B): (A) Transducer position for evaluating long head of biceps tendon stability and the subscapularis tendon in a longitudinal plane. Note the arm externally rotated and elbow flexed at 90°. (B) Medial subluxation of the biceps tendon with an empty intertubercular groove (arrow) suggestive of biceps instability. LT: Lesser tuberosity
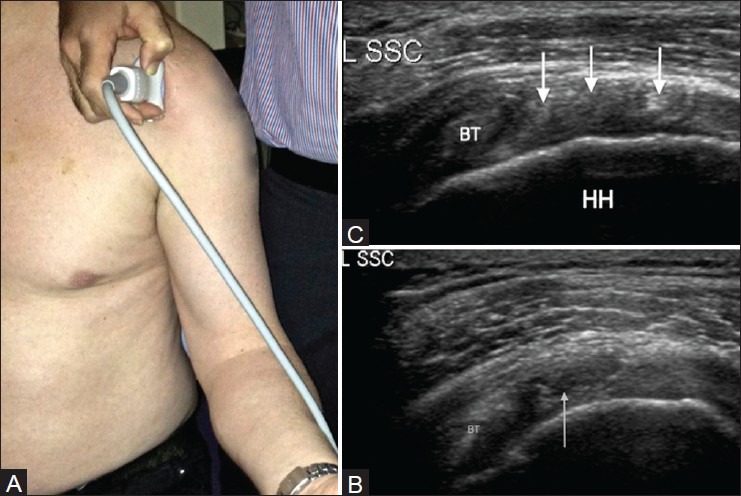
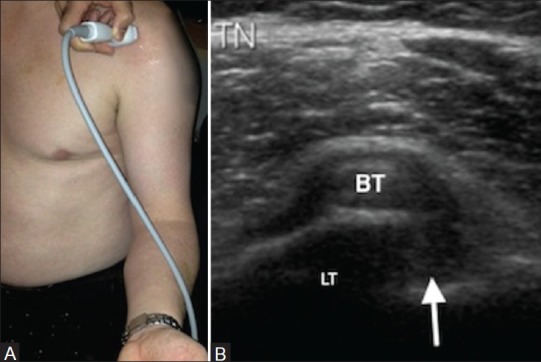
(A-C): (A) Transducer position for a transverse image of the subscapularis tendon. (B) Corresponding transverse image of the subcapularis tendon. Note the hyperechoic tendon slips (arrows) between the hypoechoic muscle fibers. (C) Short-axis view of the subscapularis tendon with a partial-thickness articular surface tear in its superior part (arrow). Biceps tendon seen on the left of the image. L SSC: Left subscapularis, BT: Biceps tendon, HH: Humeral head
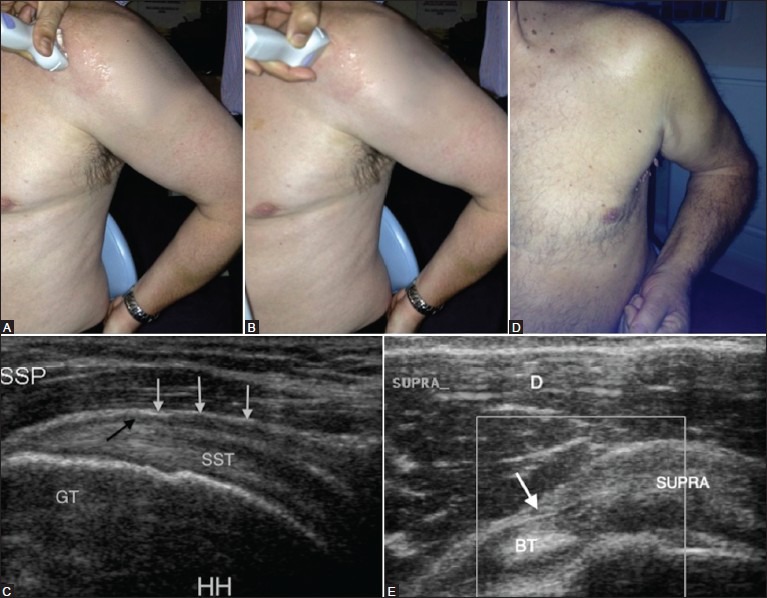
(A-E): Supraspinatus tendon (SST). Transducer placement for supraspinatus tendon in long-axis (A) and short-axis (B) with the hand on the back pocket. Longitudinal view of the SST (C) with overlying thin hypoechoic line (black arrow) representing subacromial subdeltoid bursa and the overlying subdeltoid fat (white arrows). Elbow backward position (F) to see the anterior border of supraspinatus tendon in transverse plane (E) with the echogenic component of biceps tendon sling, coracohumeral ligament (arrow). GT: Greater tuberosity, HH: humeral head, D: Deltoid muscle
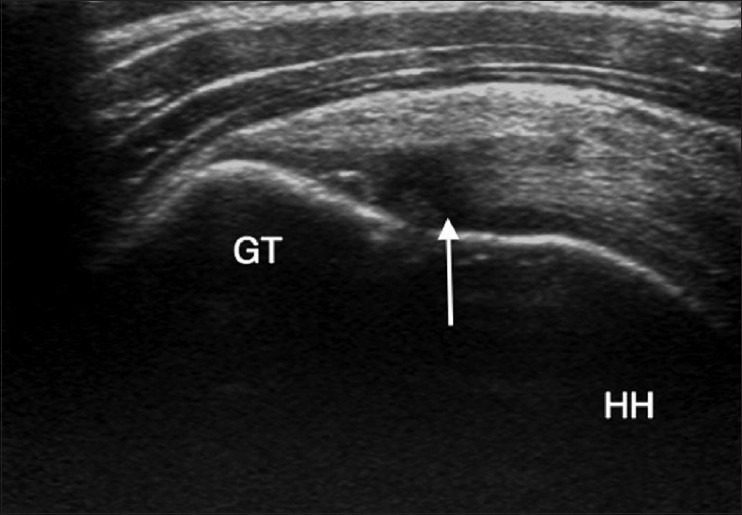
Longitudinal view of the supraspinatus tendon with an area of reduced echogenicity due to anisotrophy, at the site of tendon insertion over the greater tuberosity, which is not to be confused with a tear. HH: Humeral head
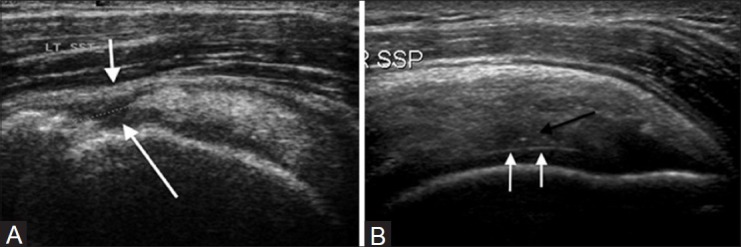
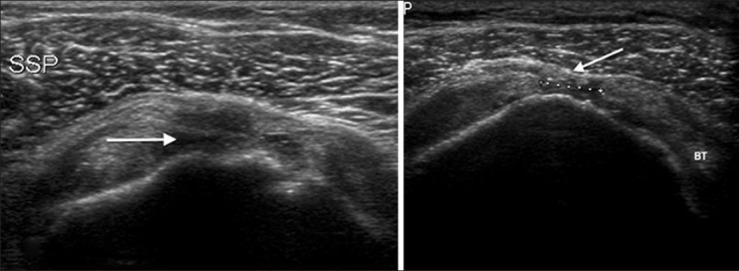
(A) Longitudinal view of supraspinatus tendon (SSP). Full-thickness tear of the tendon (long arrow) that reaches from the bursal to the articular margin with sagging of the overlying bursa (short arrow). (B) Long-axis view of the right SSP. Partial thickness articular surface tear (black arrow) and a bright anterior aspect of humeral cartilage (white arrow) – Cartilage interface sign
(A) Full-thickness tear (arrow) in anterior free edge of supraspinatus tendon. Tiny echogenic shadows due to blood particles (thin arrow) are seen to move on dynamic compression. Note irregularity over the greater tuberosity (arrowhead). (B) Short-axis view of left supraspinatus tendon. There is a full-thickness tear in the mid-portion of the tendon (between the markers) with sagging of the overlying bursa (arrow). BT: Biceps tendon
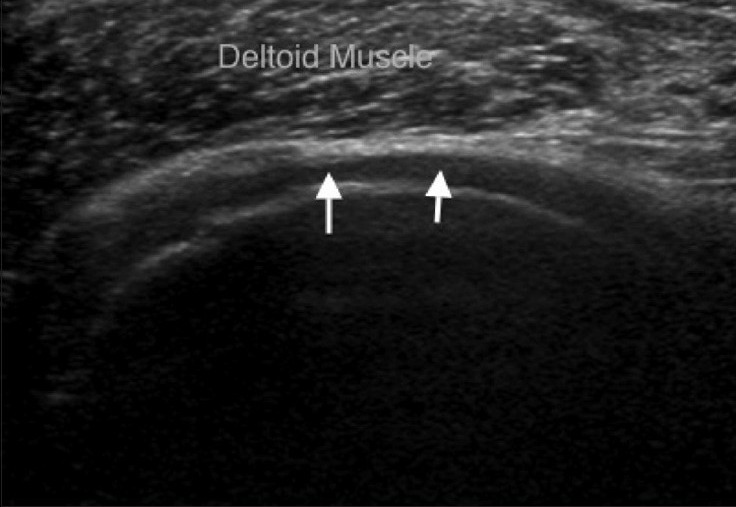
Short-axis view of supraspinatus tendon. There is a massive tear of the tendon with the deltoid muscle lying directly on the humeral head cartilage (arrows)
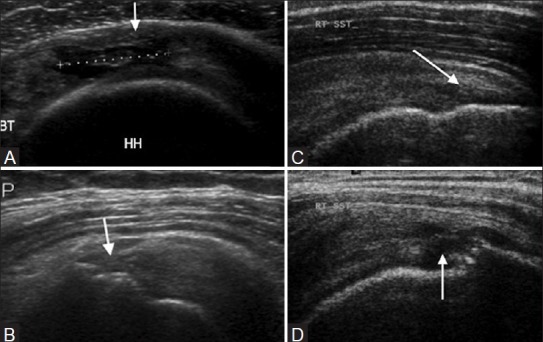
Partial-thickness tear of supraspinatus tendon. (A) Short-axis view. There is a partial-thickness articular surface tear in the mid-substance of the tendon (between markers) with a few intact fibers overlying (arrow). (B) Partial-thickness bursal surface tear (arrow) of the supraspinatus tendon. (C) Partial-thickness intrasubstance tear (arrow). (D) Partial tear (rim rent) of supraspinatus tendon at greater tuberosity (arrow). BT: Biceps tendon, HH: Humeral head
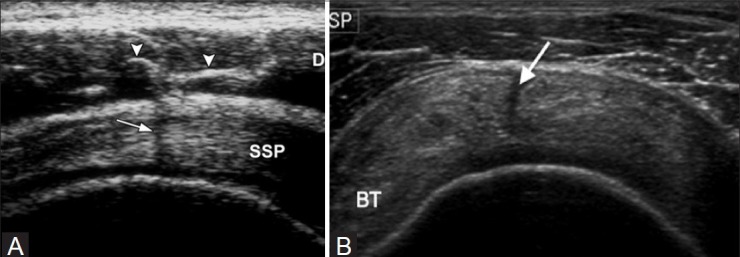
(A) Deltoid septum. Short-axis US scan of the supraspinatus tendon in a normal volunteer shows hyperechoic lines (arrowheads) in the deltoid muscle (D), which represent septa of connective tissue. A posterior acoustic shadow (arrow) may appear when the insonating beam is perpendicular to the septa. (Reprinted by permission: Figure 5, Rutten M JCM, Jager G J, Blickman J G: US of the rotator cuff: pitfalls, limitations, and artifacts. Radiographics 2006;26:589-604). (B) Tear (arrow) through the supraspinatus tendon substance
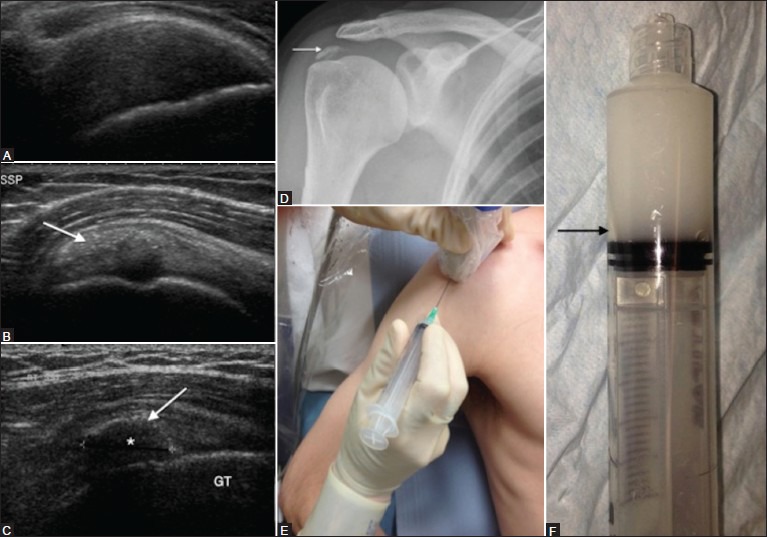
Tendon inhomogeneity. Supraspinatus tendinosis (A). The tendon is thickened and has reduced echogenicity. Long-axis view of SST showing soft (B) and hard (C) calcification (arrow) without posterior shadowing. Note the shadow (*) behind the hard calcification. Right shoulder Anteroposterior (AP) radiograph (D) with dense supraspinatus calcification (arrow). Probe placement for ultrasound-guided aspiration (E) and lavage of tendon calcification. Patient in semi-inclined position with arm behind the back. Calcium aspirate mixed with lignocaine (F) with a layer of calcium deposit (black arrow)
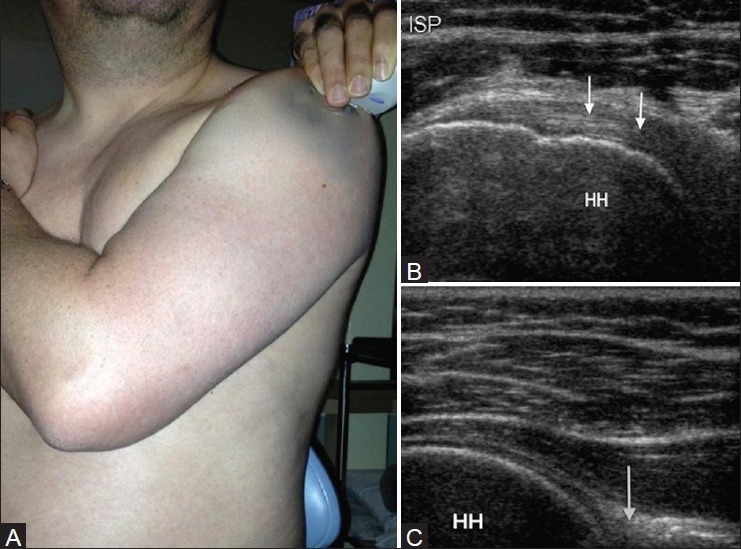
Infraspinatous tendon. (A) Probe placement over the posterior aspect of the shoulder for examination of infraspinatous tendon (long-axis), posterior glenohumeral joint and spinoglenoid notch. (B) Corresponding US image shows characteristic contour of the humeral head with adjacent infraspinatous tendon (arrow). (C) US image showing glenoid labrum (black arrow) and the posterior aspect of the glenohumeral joint
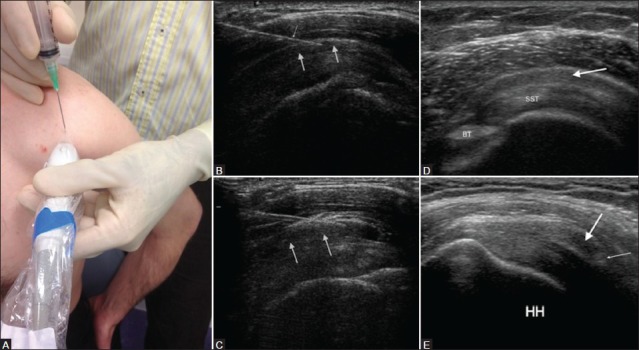
Subacromial impingement. (A) Probe placement for injecting subacromial subdeltoid bursa. Patient sitting on stool with hand on back pocket position. (B) Long-axis view of supraspinatus tendon (SST) showing needle (thin arrow) in the subacromial subdeltoid bursa (arrows) prior to injecting steroid and lignocaine mixture. (C) Expansion of the bursa (arrows) following injection. (D) Subacromial subdeltoid bursitis with thickened bursa (arrow) overlying the SST. (E) Thickening or gathering of the bursa (thick arrow) under coracoacromial ligament (thin arrow). HH: Humeral head
Similar articles
-
Shoulder ultrasound.Semin Ultrasound CT MR. 2011 Apr;32(2):101-13. doi: 10.1053/j.sult.2010.10.003. Semin Ultrasound CT MR. 2011. PMID: 21414546 Review.
-
Editorial Commentary: Is Magnetic Resonance Imaging of the Shoulder Ever Appropriate in Evaluating Patients With Calcific Tendinopathy of the Rotator Cuff?Arthroscopy. 2020 Apr;36(4):991-992. doi: 10.1016/j.arthro.2020.01.014. Arthroscopy. 2020. PMID: 32247429
-
Accuracy of shoulder ultrasound examination for diagnosis of rotator cuff pathologies: a single-center retrospective study.Ann Saudi Med. 2019 May-Jun;39(3):162-171. doi: 10.5144/0256-4947.2019.162. Epub 2019 May 30. Ann Saudi Med. 2019. PMID: 31215221 Free PMC article.
-
Normal shoulder ultrasound: anatomy and technique.Semin Musculoskelet Radiol. 2015 Jul;19(3):203-11. doi: 10.1055/s-0035-1549315. Epub 2015 May 28. Semin Musculoskelet Radiol. 2015. PMID: 26021582
-
Ultrasound of the shoulder.JBR-BTR. 2007 Sep-Oct;90(5):325-37. JBR-BTR. 2007. PMID: 18085186 Review.
Cited by
-
High-frequency Quantitative Ultrasound Imaging of Human Rotator Cuff Muscles: Assessment of Repeatability and Reproducibility.Ultrason Imaging. 2024 Jan;46(1):56-70. doi: 10.1177/01617346231207404. Epub 2023 Nov 20. Ultrason Imaging. 2024. PMID: 37981826 Free PMC article.
-
Curvelet based automatic segmentation of supraspinatus tendon from ultrasound image: a focused assistive diagnostic method.Biomed Eng Online. 2014 Dec 4;13:157. doi: 10.1186/1475-925X-13-157. Biomed Eng Online. 2014. PMID: 25471386 Free PMC article.
-
The Elias University Hospital Approach: A Visual Guide to Ultrasound-Guided Botulinum Toxin Injection in Spasticity: Part II-Proximal Upper Limb Muscles.Toxins (Basel). 2025 May 31;17(6):276. doi: 10.3390/toxins17060276. Toxins (Basel). 2025. PMID: 40559854 Free PMC article. Review.
-
Many patients fail to achieve MCID for PROMIS upper extremity and pain interference following nonoperative management of rotator cuff tears.JSES Int. 2023 Jul 14;7(6):2337-2343. doi: 10.1016/j.jseint.2023.06.014. eCollection 2023 Nov. JSES Int. 2023. PMID: 37969490 Free PMC article.
-
A narrative review of non-infected painful total shoulder arthroplasty: evaluation and treatment.Ann Jt. 2023 Apr 30;8:16. doi: 10.21037/aoj-22-43. eCollection 2023. Ann Jt. 2023. PMID: 38529254 Free PMC article. Review.
References
-
- Smith TO, Back T, Toms AP, Hing CB. Diagnostic accuracy of ultrasound for rotator cuff tears in adults: A systematic review and meta-analysis. Clin Radiol. 2011;66:1036–48. - PubMed
-
- Middleton WD, Teefey SA, Yamaguchi K. Sonography of the rotator cuff: Analysis of interobserver variability. AJR Am J Roentgenol. 2004;183:1465–8. - PubMed
-
- O’Connor PJ, Rankine J, Gibbon WW, Richardson A, Winter F, Miller JH. Interobserver variation in sonography of the painful shoulder. J Clin Ultrasound. 2005;33:53–6. - PubMed
-
- McNally EG, Rees JL. Imaging in shoulder disorders. Skeletal Radiol. 2007;36:1013–6. - PubMed
-
- Moosikasuwan JB, Miller TT, Burke BJ. Rotator cuff tears: Clinical, radiographic, and US findings. Radiographics. 2005;25:1591–607. - PubMed
