

Long-term effects of an educational seminar on antibiotic prescribing by GPs: a randomised controlled trial
- PMID: 23834882
- PMCID: PMC3693802
- DOI: 10.3399/bjgp13X669176
Long-term effects of an educational seminar on antibiotic prescribing by GPs: a randomised controlled trial
Abstract
Background: High levels of outpatient antibiotic use remain observed in many European countries. Several studies have shown a strong relationship between antibiotic use and bacterial resistance.
Aim: To assess the long-term effect of a standardised educational seminar on antibiotic prescriptions by GPs.
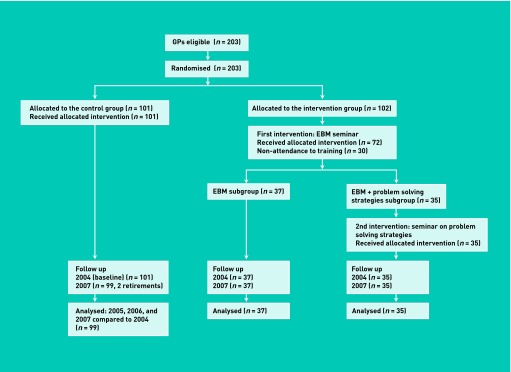
Design and setting: Randomised controlled trial of 171 GPs (of 203 initially randomised) in France.
Method: GPs in the control group (n = 99) received no antibiotic prescription recommendation. Intervention group GPs (n = 72) attended an interactive seminar presenting evidence-based guidelines on antibiotic prescription for respiratory infections. The proportion of prescriptions containing an antibiotic in each group and related costs were compared to the baseline up to 30 months following the intervention. Data were obtained from the National Health Insurance System database.
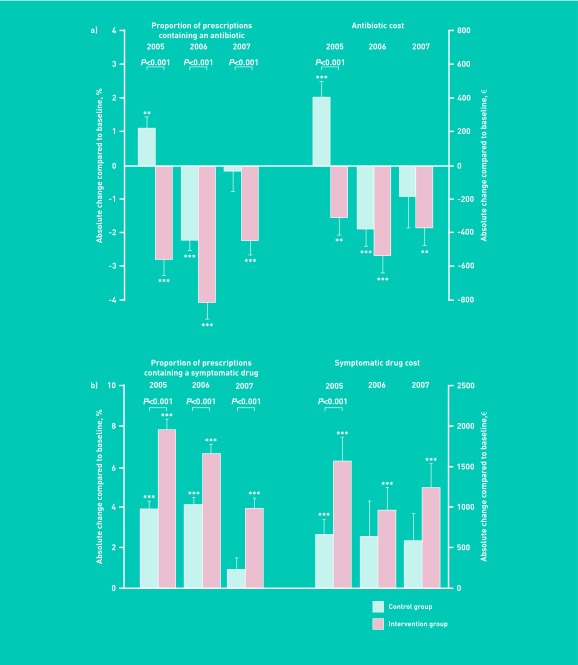
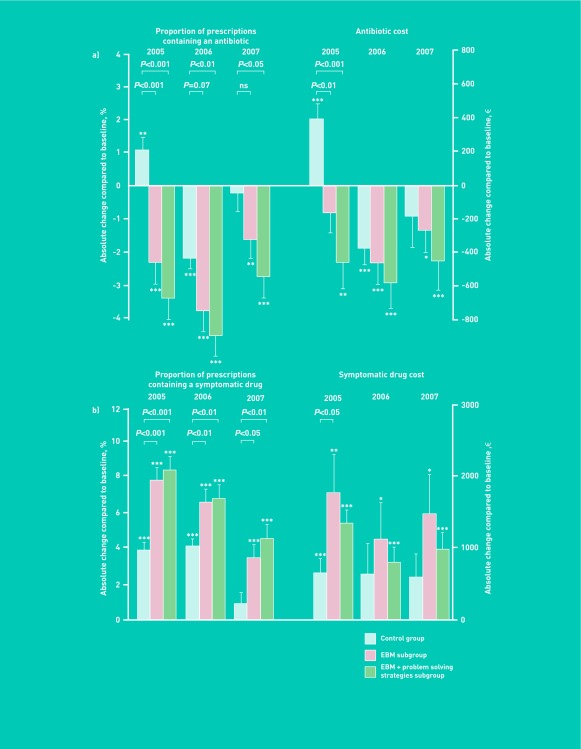
Results: In the intervention group, 4-6 months after the intervention, there was a significant decrease in the proportion of prescriptions containing an antibiotic from 15.2 ± 5.4% to 12.3 ± 5.8% (-2.8% [95% CI = -3.8 to -1.9], P<0.001). By contrast, an increase was observed in controls from 15.3 ± 6.0 to 16.4 ± 6.7% (+1.1% [95% CI = +0.4 to +1.8], P<0.01), resulting in a between-group difference of 3.93% ([95% CI = 2.75 to 5.11], P<0.001). The between-group difference was maintained 30 months after intervention (1.99% [95% CI = 0.56 to 3.42], P<0.01). Persistence of the intervention effect over the entire study period was confirmed in a hierarchical multivariate analysis.
Conclusion: This randomised trial shows that a standardised and interactive educational seminar results in a long-term reduction in antibiotic prescribing and could justify a large-scale implementation of this intervention.
Figures
References
-
- Goossens H, Ferech M, Vander Stichele R, et al. Outpatient antibiotic use in Europe and association with resistance: a cross-national database study. Lancet. 2005;365(9459):579–587. - PubMed
-
- Costelloe C, Metcalfe C, Lovering A, et al. Effect of antibiotic prescribing in primary care on antimicrobial resistance in individual patients: systematic review and meta-analysis. BMJ. 2010;340:c2096. - PubMed
-
- Elseviers MM, Ferech M, Vander Stichele RH, et al. Antibiotic use in ambulatory care in Europe (ESAC data 1997–2002): trends, regional differences and seasonal fluctuations. Pharmacoepidemiol Drug Saf. 2007;16(1):115–123. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical