

Cyclodextrin protects podocytes in diabetic kidney disease
- PMID: 23835338
- PMCID: PMC3806621
- DOI: 10.2337/db13-0399
Cyclodextrin protects podocytes in diabetic kidney disease
Abstract
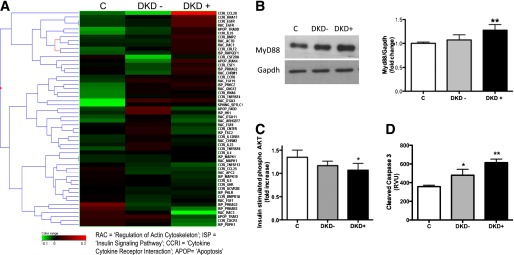
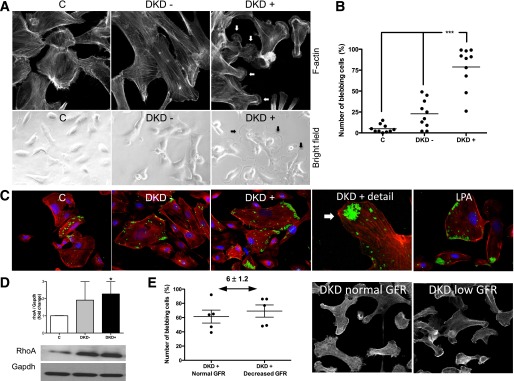
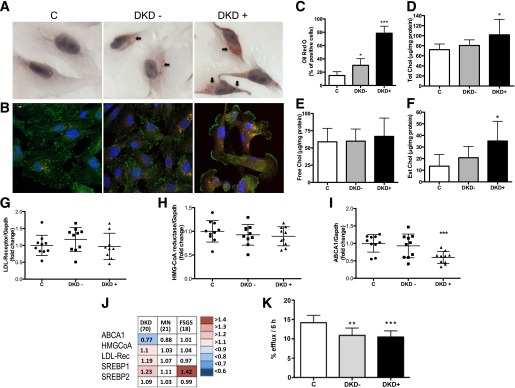
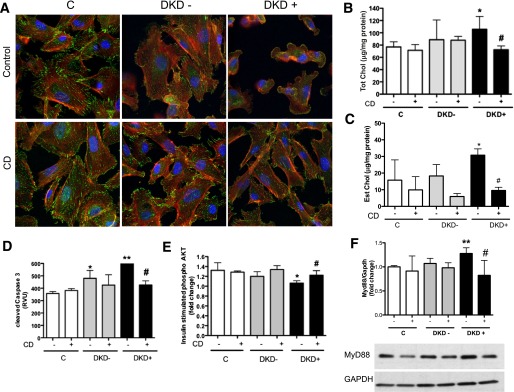
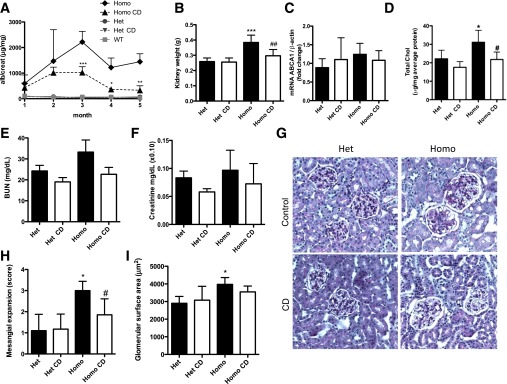
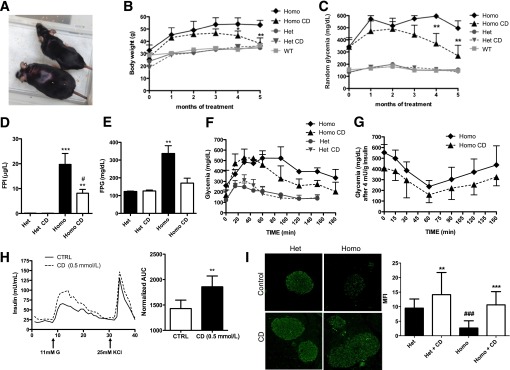
Diabetic kidney disease (DKD) remains the most common cause of end-stage kidney disease despite multifactorial intervention. We demonstrated that increased cholesterol in association with downregulation of ATP-binding cassette transporter ABCA1 occurs in normal human podocytes exposed to the sera of patients with type 1 diabetes and albuminuria (DKD(+)) when compared with diabetic patients with normoalbuminuria (DKD(-)) and similar duration of diabetes and lipid profile. Glomerular downregulation of ABCA1 was confirmed in biopsies from patients with early DKD (n = 70) when compared with normal living donors (n = 32). Induction of cholesterol efflux with cyclodextrin (CD) but not inhibition of cholesterol synthesis with simvastatin prevented podocyte injury observed in vitro after exposure to patient sera. Subcutaneous administration of CD to diabetic BTBR (black and tan, brachiuric) ob/ob mice was safe and reduced albuminuria, mesangial expansion, kidney weight, and cortical cholesterol content. This was followed by an improvement of fasting insulin, blood glucose, body weight, and glucose tolerance in vivo and improved glucose-stimulated insulin release in human islets in vitro. Our data suggest that impaired reverse cholesterol transport characterizes clinical and experimental DKD and negatively influences podocyte function. Treatment with CD is safe and effective in preserving podocyte function in vitro and in vivo and may improve the metabolic control of diabetes.
Figures
Comment in
-
Cholesterol accumulation in podocytes: a potential novel targetable pathway in diabetic nephropathy.Diabetes. 2013 Nov;62(11):3661-2. doi: 10.2337/db13-1167. Diabetes. 2013. PMID: 24158993 Free PMC article. No abstract available.
References
-
- U.S. Renal Data System USRDS 2011 Annual Data Report: Atlas of Chronic Kidney Disease and End-Stage Renal Disease in the United States. Bethesda, MD, National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, 2011
-
- Gaede P, Lund-Andersen H, Parving HH, Pedersen O. Effect of a multifactorial intervention on mortality in type 2 diabetes. N Engl J Med 2008;358:580–591 - PubMed
-
- Hovind P, Tarnow L, Rossing K, et al. Decreasing incidence of severe diabetic microangiopathy in type 1 diabetes. Diabetes Care 2003;26:1258–1264 - PubMed
-
- Somlo S, Mundel P. Getting a foothold in nephrotic syndrome. Nat Genet 2000;24:333–335 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
