

Evaluation of hybrid inverse planning and optimization (HIPO) algorithm for optimization in real-time, high-dose-rate (HDR) brachytherapy for prostate
- PMID: 23835384
- PMCID: PMC5714541
- DOI: 10.1120/jacmp.v14i4.4198
Evaluation of hybrid inverse planning and optimization (HIPO) algorithm for optimization in real-time, high-dose-rate (HDR) brachytherapy for prostate
Abstract
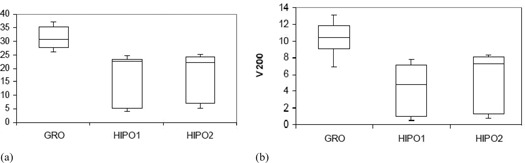
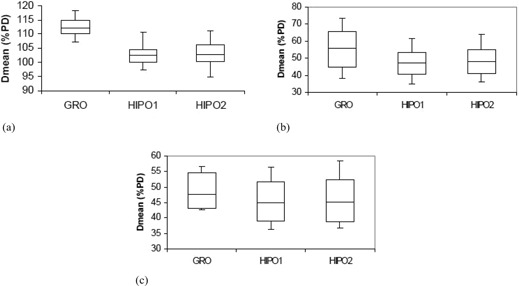
The purpose of this study is to investigate the effectiveness of the HIPO planning and optimization algorithm for real-time prostate HDR brachytherapy. This study consists of 20 patients who underwent ultrasound-based real-time HDR brachytherapy of the prostate using the treatment planning system called Oncentra Prostate (SWIFT version 3.0). The treatment plans for all patients were optimized using inverse dose-volume histogram-based optimization followed by graphical optimization (GRO) in real time. The GRO is manual manipulation of isodose lines slice by slice. The quality of the plan heavily depends on planner expertise and experience. The data for all patients were retrieved later, and treatment plans were created and optimized using HIPO algorithm with the same set of dose constraints, number of catheters, and set of contours as in the real-time optimization algorithm. The HIPO algorithm is a hybrid because it combines both stochastic and deterministic algorithms. The stochastic algorithm, called simulated annealing, searches the optimal catheter distributions for a given set of dose objectives. The deterministic algorithm, called dose-volume histogram-based optimization (DVHO), optimizes three-dimensional dose distribution quickly by moving straight downhill once it is in the advantageous region of the search space given by the stochastic algorithm. The PTV receiving 100% of the prescription dose (V100) was 97.56% and 95.38% with GRO and HIPO, respectively. The mean dose (D(mean)) and minimum dose to 10% volume (D10) for the urethra, rectum, and bladder were all statistically lower with HIPO compared to GRO using the student pair t-test at 5% significance level. HIPO can provide treatment plans with comparable target coverage to that of GRO with a reduction in dose to the critical structures.
Figures







Similar articles
-
Comparison of dose and catheter optimization algorithms in prostate high-dose-rate brachytherapy.Brachytherapy. 2016 Jan-Feb;15(1):102-11. doi: 10.1016/j.brachy.2015.09.010. Epub 2015 Nov 7. Brachytherapy. 2016. PMID: 26561276
-
A comparison of inverse optimization algorithms for HDR/PDR prostate brachytherapy treatment planning.Brachytherapy. 2015 Mar-Apr;14(2):279-88. doi: 10.1016/j.brachy.2014.09.006. Epub 2014 Oct 22. Brachytherapy. 2015. PMID: 25447341
-
Investigating the role of constrained CVT and CVT in HIPO inverse planning for HDR brachytherapy of prostate cancer.Med Phys. 2019 Jul;46(7):2955-2968. doi: 10.1002/mp.13564. Epub 2019 Jun 5. Med Phys. 2019. PMID: 31055834
-
Use of three-dimensional radiation therapy planning tools and intraoperative ultrasound to evaluate high dose rate prostate brachytherapy implants.Int J Radiat Oncol Biol Phys. 1999 Feb 1;43(3):571-8. doi: 10.1016/s0360-3016(98)00420-9. Int J Radiat Oncol Biol Phys. 1999. PMID: 10078639 Review.
-
Keeping your best options open with AI-based treatment planning in prostate and cervix brachytherapy.Brachytherapy. 2024 Mar-Apr;23(2):188-198. doi: 10.1016/j.brachy.2023.10.005. Epub 2024 Feb 1. Brachytherapy. 2024. PMID: 38296658 Review.
Cited by
-
Comparative analysis of dosimetric and radiobiological models of IPSA and HIPO algorithms in combined intra-cavitary/interstitial brachytherapy for cervical cancer.J Contemp Brachytherapy. 2023 Jun;15(3):212-219. doi: 10.5114/jcb.2023.128894. Epub 2023 Jun 23. J Contemp Brachytherapy. 2023. PMID: 37425198 Free PMC article.
-
Analysis of treatment planning time and optimization parameters for inverse planning for intracavitary and interstitial brachytherapy in uterine cervical cancer.J Appl Clin Med Phys. 2025 Jul;26(7):e70157. doi: 10.1002/acm2.70157. J Appl Clin Med Phys. 2025. PMID: 40657692 Free PMC article.
-
Investigation of Dosimetric Evaluation and Treatment Planning Time of Inverse Planning Optimization in Combined Intracavitary and Interstitial Brachytherapy for Cervical Cancer.Cureus. 2025 May 1;17(5):e83330. doi: 10.7759/cureus.83330. eCollection 2025 May. Cureus. 2025. PMID: 40452691 Free PMC article.
-
Comparison of the IPSA and HIPO algorithms for interstitial tongue high-dose-rate brachytherapy.PLoS One. 2018 Oct 4;13(10):e0205229. doi: 10.1371/journal.pone.0205229. eCollection 2018. PLoS One. 2018. PMID: 30286187 Free PMC article.
-
[Dosimetric analysis of different optimization algorithms for three-dimensional brachytherapy for gynecologic tumors].Nan Fang Yi Ke Da Xue Xue Bao. 2024 Apr 20;44(4):773-779. doi: 10.12122/j.issn.1673-4254.2024.04.20. Nan Fang Yi Ke Da Xue Xue Bao. 2024. PMID: 38708512 Free PMC article. Chinese.
References
-
- Lachance B, Béliveau‐Nadeau D, Lessard E et al. Early clinical experience with anatomy‐based inverse planning dose optimization for high‐dose‐rate boost of the prostate. Int J Radiat Oncol Biol Phys. 2002;54(1):86–100. - PubMed
-
- Demanes DJ, Rodriguez RR, Schour L, Brandt D, Altieri G. High‐dose‐rate intensity‐modulated brachytherapy with external beam radiotherapy for prostate cancer: California endocurietherapy's 10‐year results. Int J Radiat Oncol Biol Phys. 2005;61(5):1306–16. - PubMed
-
- Tang JI, Williams SG, Tai KH, Dean J, Duchesue GM. A prospective dose escalation trial of high‐dose‐rate brachytherapy boost for prostate cancer: evidence of hypofractionation efficacy? Brachytherapy. 2006;5(4):256–61. - PubMed
-
- Lessard E and Pouliot J. Inverse planning anatomy‐based dose optimization for HDR‐brachytherapy of the prostate using fast simulated annealing algorithm and dedicated objective function. Med Phys. 2001;28(5):773–79. - PubMed
-
- Lahans M. Anatomy‐based three‐dimensional dose optimization in brachytherapy using multiobjective genetic algorithms. Med Phys. 1999;26(9):1904–18. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
