

Apoptosis and dysfunction of blood dendritic cells in patients with falciparum and vivax malaria
- PMID: 23835848
- PMCID: PMC3727318
- DOI: 10.1084/jem.20121972
Apoptosis and dysfunction of blood dendritic cells in patients with falciparum and vivax malaria
Abstract
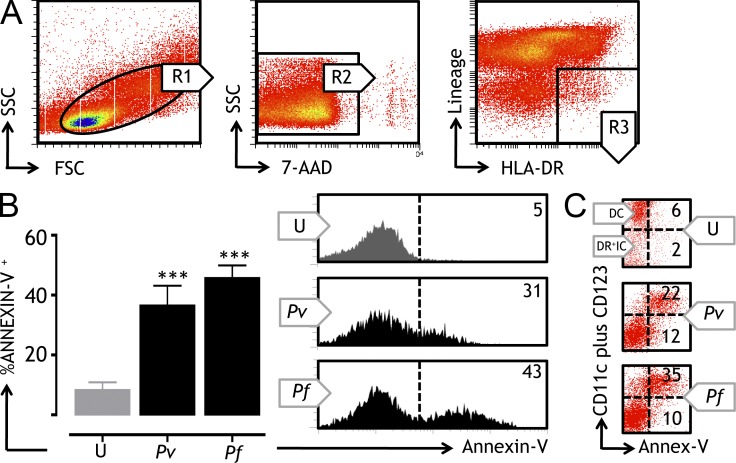
Malaria causes significant morbidity worldwide and a vaccine is urgently required. Plasmodium infection causes considerable immune dysregulation, and elicitation of vaccine immunity remains challenging. Given the central role of dendritic cells (DCs) in initiating immunity, understanding their biology during malaria will improve vaccination outcomes. Circulating DCs are particularly important, as they shape immune responses in vivo and reflect the functional status of other subpopulations. We performed cross-sectional and longitudinal assessments of the frequency, phenotype, and function of circulating DC in 67 Papuan adults during acute uncomplicated P. falciparum, P. vivax, and convalescent P. falciparum infections. We demonstrate that malaria patients display a significant reduction in circulating DC numbers and the concurrent accumulation of immature cells. Such alteration is associated with marked levels of spontaneous apoptosis and impairment in the ability of DC to mature, capture, and present antigens to T cells. Interestingly, sustained levels of plasma IL-10 were observed in patients with acute infection and were implicated in the induction of DC apoptosis. DC apoptosis was reversed upon IL-10 blockade, and DC function recovered when IL-10 levels returned to baseline by convalescence. Our data provide key information on the mechanisms behind DC suppression during malaria and will assist in developing strategies to better harness DC's immunotherapeutic potential.
Figures







References
-
- Arama C., Giusti P., Boström S., Dara V., Traore B., Dolo A., Doumbo O., Varani S., Troye-Blomberg M. 2011. Interethnic differences in antigen-presenting cell activation and TLR responses in Malian children during Plasmodium falciparum malaria. PLoS ONE. 6:e18319 10.1371/journal.pone.0018319 - DOI - PMC - PubMed
-
- Bhattarai A., Ali A.S., Kachur S.P., Mårtensson A., Abbas A.K., Khatib R., Al-Mafazy A.W., Ramsan M., Rotllant G., Gerstenmaier J.F., et al. 2007. Impact of artemisinin-based combination therapy and insecticide-treated nets on malaria burden in Zanzibar. PLoS Med. 4:e309 10.1371/journal.pmed.0040309 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
