

Weighted vaginal cones for urinary incontinence
- PMID: 23836411
- PMCID: PMC7086390
- DOI: 10.1002/14651858.CD002114.pub2
Weighted vaginal cones for urinary incontinence
Abstract
Background: For a long time pelvic floor muscle training (PFMT) has been the most common form of conservative (non-surgical) treatment for stress urinary incontinence (SUI). Weighted vaginal cones can be used to help women to train their pelvic floor muscles. Cones are inserted into the vagina and the pelvic floor is contracted to prevent them from slipping out.
Objectives: The objective of this review is to determine the effectiveness of vaginal cones in the management of female urinary stress incontinence (SUI).We wished to test the following comparisons in the management of stress incontinence: 1. vaginal cones versus no treatment; 2. vaginal cones versus other conservative therapies, such as PFMT and electrostimulation; 3. combining vaginal cones and another conservative therapy versus another conservative therapy alone or cones alone; 4. vaginal cones versus non-conservative methods, for example surgery or injectables.Secondary issues which were considered included whether:1. it takes less time to teach women to use cones than it does to teach the pelvic floor exercise; 2. self-taught use is effective;3. the change in weight of the heaviest cone that can be retained is related to the level of improvement;4. subgroups of women for whom cone use may be particularly effective can be identified.
Search methods: We searched the Cochrane Incontinence Group Specialised Trials Register (searched 19 September 2012), MEDLINE (January 1966 to March 2013), EMBASE (January 1988 to March 2013) and reference lists of relevant articles.
Selection criteria: Randomised or quasi-randomised controlled trials comparing weighted vaginal cones with alternative treatments or no treatment.
Data collection and analysis: Two reviewers independently assessed studies for inclusion and trial quality. Data were extracted by one reviewer and cross-checked by the other. Study authors were contacted for extra information.
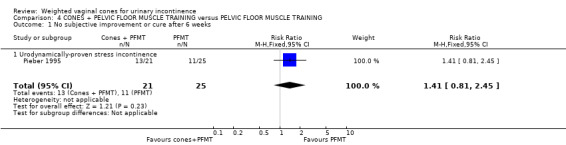
Main results: We included 23 trials involving 1806 women, of whom 717 received cones. All of the trials were small, and in many the quality was hard to judge. Outcome measures differed between trials, making the results difficult to combine. Some trials reported high drop-out rates with both cone and comparison treatments. Seven trials were published only as abstracts.Cones were better than no active treatment (rate ratio (RR) for failure to cure incontinence 0.84, 95% confidence interval (CI) 0.76 to 0.94). There was little evidence of difference for a subjective cure between cones and PFMT (RR 1.01, 95% CI 0.91 to 1.13), or between cones and electrostimulation (RR 1.26, 95% CI 0.85 to 1.87), but the confidence intervals were wide. There was not enough evidence to show that cones plus PFMT was different to either cones alone or PFMT alone. Only seven trials used a quality of life measures and no study looked at economic outcomes.Seven of the trials recruited women with symptoms of incontinence, while the others required women with urodynamic stress incontinence, apart from one where the inclusion criteria were uncertain.
Authors' conclusions: This review provides some evidence that weighted vaginal cones are better than no active treatment in women with SUI and may be of similar effectiveness to PFMT and electrostimulation. This conclusion must remain tentative until larger, high-quality trials, that use comparable and relevant outcomes, are completed. Cones could be offered as one treatment option, if women find them acceptable.
Conflict of interest statement
Peter Herbison was the co‐author of one of the included trials (Wilson 1998), and a previous author of this review, Stan Plevnik was a co‐author of two of the trials included (Peattie 1988a; Wise 1993). Stan Plevnik was the originator of the idea of weighted vaginal cones.
Figures































Update of
-
Weighted vaginal cones for urinary incontinence.Cochrane Database Syst Rev. 2002;(1):CD002114. doi: 10.1002/14651858.CD002114. Cochrane Database Syst Rev. 2002. Update in: Cochrane Database Syst Rev. 2013 Jul 08;(7):CD002114. doi: 10.1002/14651858.CD002114.pub2. PMID: 11869623 Updated.
References
References to studies included in this review
Arvonen 2001 {published and unpublished data}
-
- Arvonen T, Fianu‐Jonasson A, Tyni‐Lenné R. Effectiveness of two conservative modes of physical therapy in women with urinary stress incontinence. Neurourology and Urodynamics 2001;20:591‐9. - PubMed
Arvonen 2002 {published data only}
-
- Arvonen T, Jonasson AF, Tyni‐Lenné R. A clinical trial comparing conventional pelvic floor training and training with vaginal balls in women with stress urinary incontinence — a pilot study. Nordisk Fysioterapi 2002;6(1):41–6.
Bourcier 1994 {published data only}
-
- Bourcier A, Juras J. Randomised study comparing physiotherapy and pelvic floor rehabilitation. Proceedings of the 24th Annual Meeting of the International Continence Society; 1994 Aug 30‐Sept 3; Prague. 1994:146.
Burton 1993 {published data only}
-
- Burton G. Active vaginal cone therapy: a new form of treatment for genuine stress incontinence (abstract). Proceedings of the 23rd Annual Meeting of the International Continence Society (Conference proceedings: Read by title). 1993:A134.
Bø 1999 {published and unpublished data}
-
- Bø K, Talseth T. Single blind randomised controlled trial on the effect of pelvic floor muscle strength training, electrical stimulation, cones or control on severe genuine stress incontinence. Abstract 87. Neurourology and Urodynamics 1998;17(4):421‐2.
Cammu 1998 {published data only}
-
- Cammu H, Nylen M. Pelvic floor exercises (PFE) versus vaginal cones (VC) in the treatment of genuine stress incontinence (Abstract number 225). Proceedings of the 26th Annual Conference of the International Continence Society; 1996 Aug 27‐30; Athens, Greece. 1996:223.
-
- Cammu H, Nylen M. Pelvic floor exercises versus vaginal weight cones in genuine stress incontinence. European Journal of Obstetrics Gynecology and Reproductive Biology 1998;77:89‐93. - PubMed
Castro 2008 {published data only}
Delneri 2000 {published data only}
-
- Delneri C, Benedetto P. Pelvic floor rehabilitation. A comparison of two methods of treatment: vaginal cones versus functional electrical stimulation. Europa Medicophysica 2000;36:45‐8.
Gameiro 2010 {published data only}
-
- Gameiro MO, Moreira EH, Gameiro FO, Moreno JC, Padovani CR, Amaro JL. Vaginal weight cone versus assisted pelvic floor muscle training in the treatment of female urinary incontinence. A prospective, single‐blind, randomized trial. International Urogynecology Journal 2010;21(4):395‐9. - PubMed
-
- Moreira E, Orsi Gameiro M, Fugita OEH, Kawano PR, Yamamoto HA, Amaro JL. Vaginal weight cone versus assisted pelvic floor muscle training in the treatment of female urinary incontinence. A prospective, single‐blind, randomized trial (Abstract 1703). The Journal of Urology 2009;181(4, Supplement):614. - PubMed
Haken 1991 {published data only}
-
- Haken J, Benness C, Cardozo L, Cutner A. A randomised trial of vaginal cones and pelvic floor exercises in the management of genuine stress incontinence. Abstract 76. Neurourology & Urodynamics 1991;10(4):393‐4.
Harvey 2006 {published data only}
-
- Harvey M‐A, Johnston SL. A randomized, single‐blind, prospective trial comparing pelvic floor physiotherapy with biofeedback versus weighted vaginal cones in the treatment of female genuine stress urinary incontinence: a pilot study (Abstract 318). International Urogynecology Journal 2006;17(Suppl 2):S235‐S236.
Laycock 1993 {published data only}
-
- Laycock J, Jerwood D. Does pre‐modulated interferential therapy cure genuine stress incontinence?. Physiotherapy 1993;79(8):553‐60.
Laycock 2001 {published data only}
-
- Laycock J, Brown J, Cusack C, Green S, Jerwood D, Mann K, et al. A multi‐centre, prospective, randomised, controlled, group comparative study of the efficacy of vaginal cones and PFX. Abstract 47. Neurourology and Urodynamics 1999;18(4):301‐2.
-
- Laycock J, Brown J, Cusack C, Green S, Jerwood D, Mann K, et al. A multicentre, prospective, randomised, controlled, group comparative study of the efficacy of vaginal cones and PFX (Abstract). International Urogynecology Journal and Pelvic Floor Dysfunction 1999;10(Suppl 1):S49.
-
- Laycock J, Brown J, Cusack C, Green S, Jerwood D, Mann K, et al. Pelvic floor reeducation for stress incontinence: comparing three methods. British Journal of Community Nursing 2001;6(5):230‐7. - PubMed
Olah 1990 {published data only}
-
- Bridges N, Denning J, Olah KS, Farrar DJ. A prospective trial comparing interferential therapy and treatment using cones in patients with symptoms of stress incontinence. Abstract 73. Neurourology and Urodynamics 1988;7(3):267‐8.
-
- Olah KS, Bridges N, Denning J, Farrar DJ. The conservative management of patients with symptoms of stress incontinence: a randomized prospective study comparing weighted vaginal cones and interferential therapy. American Journal of Obstetrics and Gynecology 1990;162:87‐92. - PubMed
Peattie 1988a {published and unpublished data}
-
- Peattie A, Plevnik S. Cones versus physiotherapy as conservative management of genuine stress incontinence. Abstract 72. Neurourology and Urodynamics 1988;7(3):265‐6.
-
- Peattie AB, Taylor B, Plevnik S, Stanton SL. Cones versus physiotherapy for conservative treatment of genuine stress incontinence (Abstract number 169). Proceedings of the Silver Jubilee British Congress of Obstetrics and Gynaecology. London, 1989 Jul 4‐7.
Pereira 2012 {published data only}
-
- Pereira VS, Melo MV, Correia GN, Driusso P. Long‐term effects of pelvic floor muscle training with vaginal cone in post‐menopausal women with urinary incontinence: a randomized controlled trial. Neurourology and Urodynamics 2013;32:48–52. - PubMed
-
- Pereira VS, Melo MV, Correia GN, Driusso P. Vaginal cone for postmenopausal women with stress urinary incontinence: randomized, controlled trial. Climacteric 2012;15:45–51. - PubMed
Pieber 1995 {published data only}
-
- Pieber D, Zivkovic F, Tamussino K. Pelvic floor exercises alone or with vaginal cones in premenopausal women with mild to moderate stress incontinence [Beckenbodengymnastik allien oder mit vaginalkonin bei prämenopausalen frauen mit milder und mässiger stressharninkontinenz]. Gynäkologisch‐Geburtshilfliche Rundschau 1994;34:32‐3. - PubMed
-
- Pieber D, Zivkovic F, Tamussino K, Ralph G. Pelvic floor exercise alone or with vaginal cones for the treatment of mild and moderate stress incontinence in premenopausal women: a randomised trial (Abstract). Proceedings of the 24th Annual Meeting of the International Continence Society; 1994 Aug 27‐Sept 2; Prague (Czech Republic) (Conference proceedings: Read by title). 1994:162.
-
- Pieber D, Zivkovic F, Tamussino K, Ralph G, Lippitt G, Fauland B. Pelvic floor exercise alone or with vaginal cones for the treatment of mild to moderate stress urinary incontinence in premenopausal women. International Urogynecology Journal 1995;6:14‐7.
Santos 2009 {published data only}
-
- Santos PFD, Oliveira E, Zanetti MRD, Arruda RM, Sartori MGF, Girão MJBC, et al. Electrical stimulation of the pelvic floor versus vaginal cone therapy for the treatment of stress urinary incontinence [Eletroestimulação funcional do assoalho pélvico versus terapia com os cones vaginais para o tratamento de incontinência urinária de esforço (Portuguese)]. Revista Brasileira de Ginecologia e Obstetríca 2009;31(9):447‐52. - PubMed
Seo 2004 {published data only}
-
- Seo JT, Yoon H, Kim YH. A randomized prospective study comparing new vaginal cone and FES‐Biofeedback. Yonsei Medical Journal 2004;45(5):879‐84. - PubMed
Terry 1996 {published data only}
-
- Terry PB, White SM. Randomised trial comparing Enhance with physiotherapy for the treatment of GSI. Proceedings of the 26th Annual Meeting of the International Continence Society; 1996 Aug 27‐30; Athens (Greece). 1996:248‐9.
Williams 2006 {published and unpublished data}
-
- Williams K, Coleby D, Abrams K, Shaw C, Assassa P, McGrouther C. Randomised controlled trial of the clinical effectiveness of services for urinary symptoms: six year follow‐up (Abstract number 45). Neurourology and Urodynamics 2007;26(5):660‐1.
-
- Williams KS, Assassa RP, Gillies CL, Abrams KR, Turner DA, Shaw C et al and the Leicestershire MRC Incontinence Study Team. A randomized controlled trial of the effectiveness of pelvic floor therapies for urodynamic stress and mixed incontinence. BJU International 2006;98:1043‐50. - PubMed
Wilson 1998 {published and unpublished data}
-
- Wilson PD, Herbison GP. A randomized controlled trial of pelvic floor muscle exercises to treat postnatal urinary incontinence. International Urogynecology Journal 1998;9:257‐64. - PubMed
Wise 1993 {published data only}
-
- Wise BG, Haken J, Cardozo LD, Plevnik S. A comparative study of vaginal cone therapy, cones + Kegel exercises, and maximal electrical stimulation in the treatment of female genuine stress incontinence. Abstract 76. Neurourology and Urodynamics 1993;12(4):436‐7.
References to studies excluded from this review
Delgado 2010 {published data only}
-
- Delgado D, Drake M. A randomised controlled trial of the Pelvic Toner Device in female stress urinary incontinence. British Journal of Urology International 21 September 2010;www2.bjui.org/ContentFullitem.aspx?id=427&SectionType=4:1–7 (last accessed 18 June 2013). [Web only publication] - PubMed
Ferreira 2011 {published data only}
-
- Ferreira M, Santos P. Pelvic floor muscle training programmes: a systematic review [Nos programas de treino dos músculos do pavimento pélvico [Portuguese]]. Acta Médica Portuguesa 2011;24:309–18. - PubMed
Jonasson 1989 {published data only}
-
- Jonasson A, Larsson B, Pschera H. Testing and training of the pelvic floor muscles after childbirth. Acta Obstetricia Gynecologica Scandinavica 1989;68:301‐4. - PubMed
Lentz 1994 {published data only}
-
- Lentz G, Plevnik S, Stanton SL. Vaginal cones versus bladder drill for sensory urgency treatment (Abstract). Proceedings of the 24th Annual Meeting of the International Continence Society (Conference proceedings: Read by title). Prague, 1994:35‐6.
Norton 1990 {published data only}
-
- Norton P, Baker J. Randomized prospective trial of vaginal cones vs. Kegel exercises in postpartum primiparous women. Abstract 85. Neurourology and Urodynamics 1990;9(4):434‐5.
Parkkinen 2004 {published data only}
-
- Parkkinen A, Karjalainen E, Vartiainen M, Penttinen J. Physiotherapy for female stress urinary incontinence: individual therapy at the outpatient clinic versus home‐based pelvic floor training: A five‐year follow‐up study. Neurourology and Urodynamics 2004;23:643‐8. - PubMed
Salinas Casado 1999 {published data only}
-
- Salinas Casado J, Virseda Charmorro M, Esteban Fuertes M. The therapeutic efficacy of vaginal cones in rehabilitating the perineal musculature. The RECOVA Group [Eficacia terapéutica de los conos vaginales en la rehabilitación de la musculatura perineal]. Archivos Espanoles de Urologia 1999;52(1):53‐60. - PubMed
Williams 2005 {published data only}
References to ongoing studies
Driusso 2010 {published data only}
-
- Driusso P, Correia GN, Pereira VS, Aveiro MC, Melo MV, Tahara N. Physiotherapy for women with stress urinary incontinence: effects of kinesiotherapy, vaginal cones and electrical stimulation. Australian New Zealand Clinical Trials Registry 25 March 2010; Vol. ACTRN12610000254099.
Additional references
Abrams 1989
-
- Abrams P, Blaivas J, Stanton S, Anderson J. The standardisation of terminology of lower urinary tract function. World Journal of Urology 1989;6:233‐45. - PubMed
Bump 1991
-
- Bump RC, Hurt WG, Fantl A, Wyman JF. Assessment of Kegel pelvic muscle exercise performance after brief verbal instruction. American Journal of Obstetrics and Gynecology 1991;165:322‐9. - PubMed
Bump 1992a
-
- Bump R, Sugerman H, Fantl J. Obesity and lower urinary tract function in women: effect of surgically induced weight loss. American Journal of Obstetrics and Gynecology 1992;167:392‐9. - PubMed
Bump 1992b
-
- Bump R, McClish D. Cigarette smoking and urinary incontinence in women. American Journal of Obstetrics and Gynecology 1992;167:1213‐8. - PubMed
Bø 1995
-
- Bø K. Vaginal weight cones. Theoretical framework, effect on pelvic floor muscle strength and female stress urinary incontinence. Acta Obstetricia Gynecologica Scandinavica 1995;74:87‐92. - PubMed
Deindl 1995
-
- Deindl FM, Schussler B, Vodusek DB, Hesse U. Neurophysiological effect of vaginal cone application in continent and urinary stress incontinent women. International Urogynecology Journal and Pelvic Floor Dysfunction 1995;6:204‐8.
Dumoulin 2010
Gameiro 2012
-
- Gameiro LFO, Dib RP, Gameiro MO, Amaro JL. Electrical stimulation with non‐implanted electrodes for overactive bladder in adults. Cochrane Database of Systematic Reviews 2012, Issue 9. [DOI: 10.1002/14651858.CD010098] - DOI
Hahn 1996
-
- Hahn I, Milsom I, Ohlsson BL, Ekelund P, Uhlemann C, Fall M. Comparative assessment of pelvic floor function using vaginal cones, vaginal digital palpatation and vaginal pressure measurements. Gynecology and Obstetric Investigation 1996;41:269‐74. - PubMed
Hanzal 1993
-
- Hanzal E, Berger E, Koelbl H. Levator ani muscle morphology and recurrent genuine stress incontinence. Obstetrics & Gynecology 1993;81:426‐9. - PubMed
Hay‐Smith 2006
Hay‐Smith 2011
Herderschee 2011
Higgins 2011
-
- Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org 2011.
Hu 1990
-
- Hu T. Impact of urinary incontinence on health‐care costs. Journal of American Geriatric Society 1990;38:292‐5. - PubMed
Jolleys 1988
Kegel 1951
-
- Kegel AH. Physiologic therapy for urinary stress incontinence. Journal of the American Medical Association 1951;146:915‐7. - PubMed
Lagro‐Janssen 1994
-
- Lagro‐Janssen AL, Smits AJ, Weel C. Beneficial effect of exercise therapy in urinary incontinence in family practice depends largely on therapy compliance and motivation. Nederlandse Tijdschrift Geneeskunde 1994;138:1273‐6. - PubMed
Miller 1996
-
- Miller J, Ashton‐Miller JA, DeLancy OL. The knack: use of precisely‐timed pelvic muscle contraction can reduce leakage in SUI. Neurourology and Urodynamics 1996;15:392‐3.
Morley 1995
-
- Morley R, Cumming J, Weller R. Morphology and neuropathology of the pelvic floor in patients with stress incontinence. International Urogynecology Journal 1995;7:3‐12. - PubMed
Peattie 1988b
-
- Peattie AB, Plevnik S, Stanton SL. Vaginal cones: a conservative method of treating genuine stress incontinence. British Journal of Obstetrics and Gynaecology 1988;95:1049‐53. - PubMed
Plevnik 1985
-
- Plevnik S. New method for testing and strengthening of pelvic floor muscles. Proceedings of the 15th Annual Meeting of the International Continence Society. London, 1985:267‐8.
Ryhammer 1999
-
- Ryhammer AM, Djurhuus JC, Laurberg S. Pad testing in incontinent women: a review. International Urogynecology Journal 1999;10:111‐5. - PubMed
Smith 1989a
-
- Smith ARB, Hosker GL, Warrell DW. The role of partial denervation of the pelvic floor in the aetiology of genitourinary prolapse and stress incontinence of urine. A neurophysiological study. British Journal of Obstetrics and Gynaecology 1989;96:24‐8. - PubMed
Smith 1989b
-
- Smith ARB, Hosker GL, Warrell DW. The role of pudendal nerve damage in the aetiology of genuine stress incontinence in women. British Journal of Obstetrics and Gynaecology 1989;96:29‐32. - PubMed
Snooks 1984
-
- Snooks SJ, Swash M, Setchell M, Henry MM. Injury to innervation of pelvic floor sphincter musculature in childbirth. Lancet 1984;2:546‐50. - PubMed
Soroka 2002
-
- Soroka D, Drutz HP, Glazener CMA, Hay‐Smith EJC, Ross SJ. Perineal pad test in evaluating outcome of treatments for female incontinence: a systematic review. International Urogynaecology Journal 2002;13(3):165‐75. - PubMed
Walters 1992
-
- Walters MD, Realini JP, Dougherty M. Nonsurgical treatment of urinary incontinence. Current Opinion in Obstetrics & Gynecology 1992;4:554‐8. - PubMed
Wilson 1996
-
- Wilson PD, Herbison RM, Herbison GP. Obstetric practice and the prevalence of urinary incontinence three months after delivery. British Journal of Obstetrics and Gynaecology 1996;103:154‐61. - PubMed
Wyman 1990
-
- Wyman JF, Harkins SW, Fantl JA. Psychosocial impact of urinary incontinence in the community‐dwelling population. Journal of American Geriatric Society 1990;38:282‐8. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical