

Systematic identification and treatment of smokers by hospital based cessation practitioners in a secondary care setting: cluster randomised controlled trial
- PMID: 23836616
- PMCID: PMC3704182
- DOI: 10.1136/bmj.f4004
Systematic identification and treatment of smokers by hospital based cessation practitioners in a secondary care setting: cluster randomised controlled trial
Abstract
Objectives: To investigate the effectiveness of the systematic default provision of smoking cessation support to all adult smokers admitted to hospital, relative to usual care.
Design: Open, cluster randomised controlled trial.
Setting: Acute medical wards in one large teaching hospital in the United Kingdom.
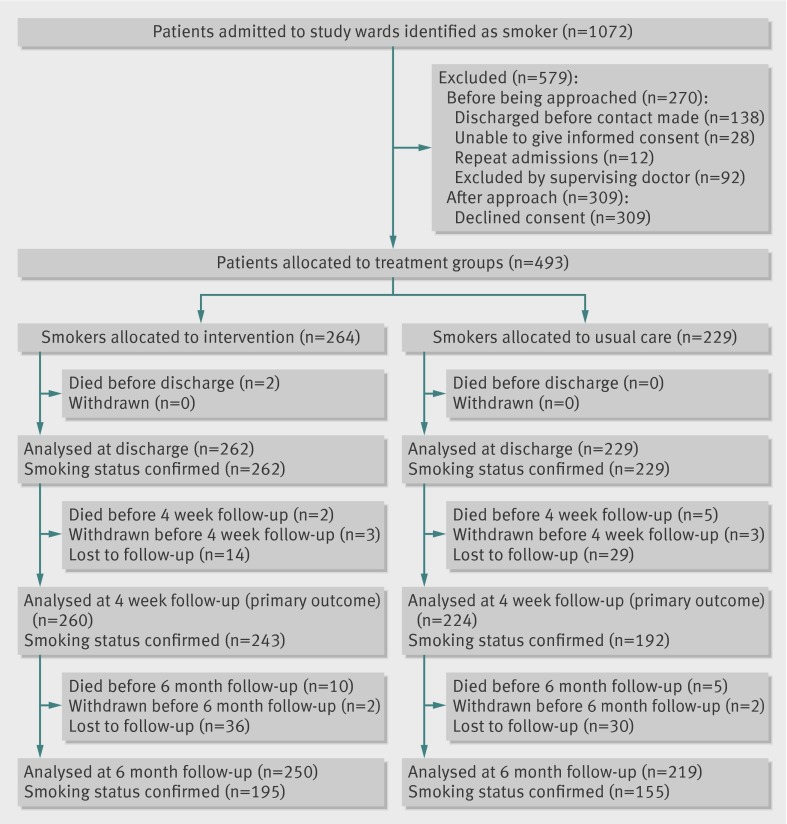
Participants: 264 patients randomised to intervention and 229 to usual care; primary outcome data were available at four weeks for 260 and 224 patients, respectively. All adult smokers and recent ex-smokers able to give informed consent were eligible for entry into the study.
Interventions: The intervention comprised systematic smoking ascertainment and default provision of behavioural support and cessation pharmacotherapy for the duration of the hospital stay for all smokers and recent ex-smokers, with follow-up and referral to community services after discharge. Usual care comprised cessation support delivered at the initiative and discretion of clinical staff. All staff and patients were aware of group assignment.
Main outcome measures: Smoking cessation at four weeks, validated by measuring exhaled carbon monoxide. Secondary outcomes were uptake of inpatient behavioural support, use of cessation pharmacotherapy, referral to and uptake of community support after discharge, and validated smoking cessation at six months. Participants lost to follow-up were assumed to have reverted to smoking.
Results: All patients in the intervention group received at least brief advice to quit smoking, compared to 106 (46%) patients in the usual care group. Cessation at four weeks was achieved by 38% (n=98) of intervention patients and 17% (n=37) of usual care patients (adjusted odds ratio 2.10 (95% confidence interval 0.96 to 4.61), P=0.06, number of patients needed to treat 8). Uptake of inpatient behavioural support, use of pharmacotherapy, and referral to and uptake of community support after discharge were all substantially and statistically significantly higher in the intervention group than in the usual care group. Cessation at six months was achieved by 19% (n=47) of intervention and 9% (n=19) of usual care patients, although this difference was not significant (adjusted odds ratio 1.53 (95% confidence interval 0.60 to 3.91); P=0.37).
Conclusions: Substantial improvements in smoking cessation among smokers admitted to hospital can be achieved by systematic ascertainment and delivery of cessation support in secondary care.
Trial registration: International Standard Randomised Controlled Trial Number ISRCTN25441641.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
References
-
- Tengs TO, Adams ME, Pliskin JS, Safran DG, Siegel JE, Weinstein MC, et al. 500 Lifesaving interventions and their cost-effectiveness. Risk Analysis 1995;15:369-90. - PubMed
-
- National Institute for Health and Clinical Excellence. Brief interventions and referral for smoking cessation in primary care and other settings. NICE, 2006.
-
- US Department of Health and Human Services Public Health Service. Treating tobacco use and dependence: 2008 update. May 2008. www.ahrq.gov/professionals/clinicians-providers/guidelines-recommendatio....
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical