

Inhaled corticosteroid use in patients with chronic obstructive pulmonary disease and the risk of pneumonia: a retrospective claims data analysis
- PMID: 23836970
- PMCID: PMC3699136
- DOI: 10.2147/COPD.S42366
Inhaled corticosteroid use in patients with chronic obstructive pulmonary disease and the risk of pneumonia: a retrospective claims data analysis
Abstract
Background: The use of inhaled corticosteroids in patients with chronic obstructive pulmonary disease (COPD) has been associated with an increased risk of pneumonia in controlled clinical trials and case-control analyses.
Objective: Using claims databases as a research model of real-world diagnosis and treatment, to determine if the use and dose of inhaled corticosteroids (ICS) among patients with newly diagnosed COPD are associated with increased risk of pneumonia.
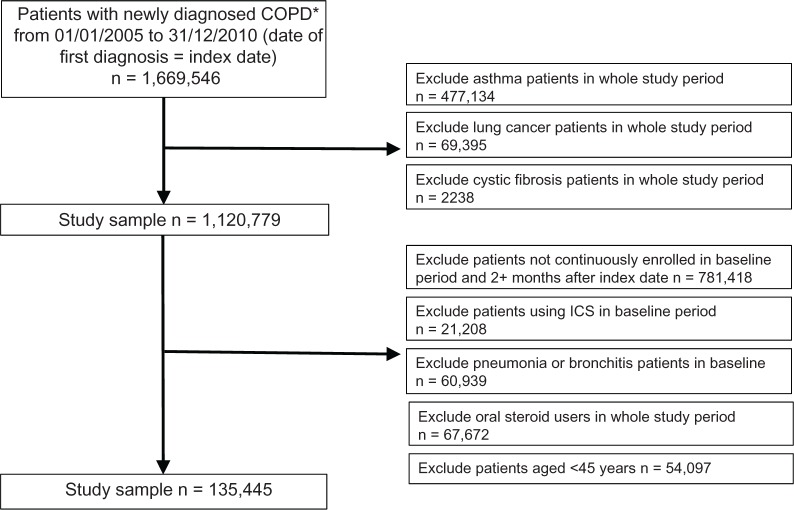
Patients and methods: This was a retrospective cohort analysis of patients diagnosed with COPD between January 01, 2006 and September 30, 2010, drawn from databases (years 2006-2010). Patients (aged ≥45 years) were followed until first pneumonia diagnosis, end of benefit enrollment, or December 31, 2010, whichever was earliest. A Cox proportional hazard model was used to assess the association of ICS use and risk of pneumonia, controlling for baseline characteristics. Daily ICS use was classified into low, medium, and high doses (1 μg-499 μg, 500 μg-999 μg, and ≥1000 μg fluticasone equivalents daily) and was modeled as a time-dependent variable.
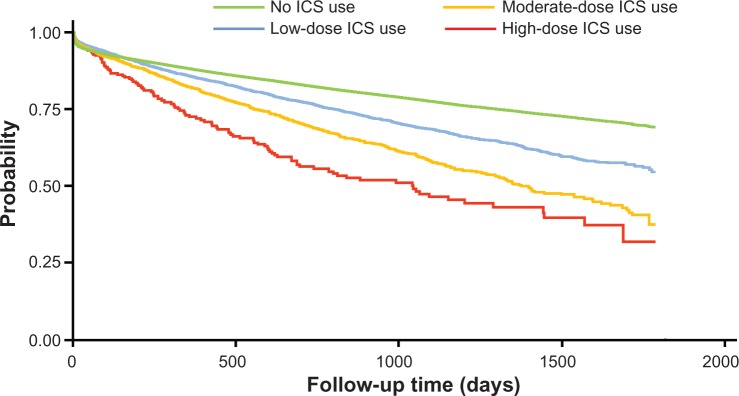
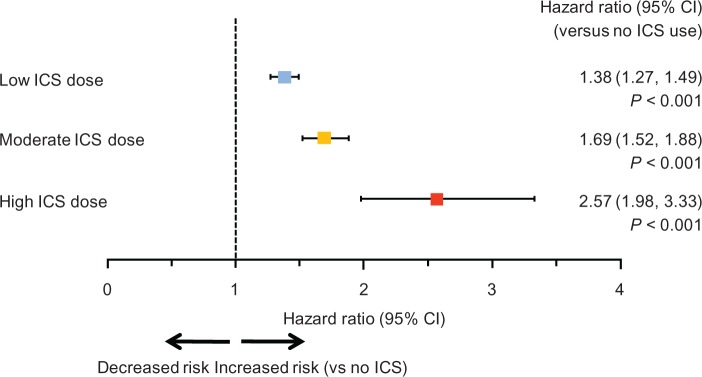
Results: Among 135,445 qualifying patients with a total of 243,097 person-years, there were 1020 pneumonia incidences out of 5677 person-years on ICS (crude incidence rate, 0.180 per person-year), and 27,730 pneumonia incidences out of 237,420 person-years not on ICS (crude incidence rate, 0.117 per person-year). ICS use was associated with a dose-related increase in risk of pneumonia, with adjusted hazard ratios (versus no use; (95% confidence interval) of 1.38 (1.27-1.49) for low-dose users, 1.69 (1.52-1.88) for medium-dose users, and 2.57 (1.98-3.33) for high-dose users (P < 0.01 versus no use and between doses).
Conclusion: The use of ICS in newly diagnosed patients with COPD is potentially associated with a dose-related increase in the risk of pneumonia.
Keywords: COPD; ICS; LABA; pneumonia.
Figures
References
-
- Asche CV, Brixner DI, Conoscenti CS, et al. Assessment of physician prescribing for primary care patients with chronic obstructive pulmonary disease (COPD) in a national electronic medical record (EMR) research database. Chest. 2006;130(4):175s. [abstract]
-
- de Miguel-Díez J, Carrasco-Garrido P, Rejas-Gutierrez J, et al. I nappropriate overuse of inhaled corticosteroids for COPD patients: impact on health costs and health status. Lung. 2011;189(3):199–206. - PubMed
-
- Mehuys E, Boussery K, Adriaens E, et al. COPD management in primary care: an observational, community pharmacy-based study. Ann Pharmacother. 2010;44(2):257–266. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
