

Beyond intracranial pressure: optimization of cerebral blood flow, oxygen, and substrate delivery after traumatic brain injury
- PMID: 23837598
- PMCID: PMC3716965
- DOI: 10.1186/2110-5820-3-23
Beyond intracranial pressure: optimization of cerebral blood flow, oxygen, and substrate delivery after traumatic brain injury
Abstract
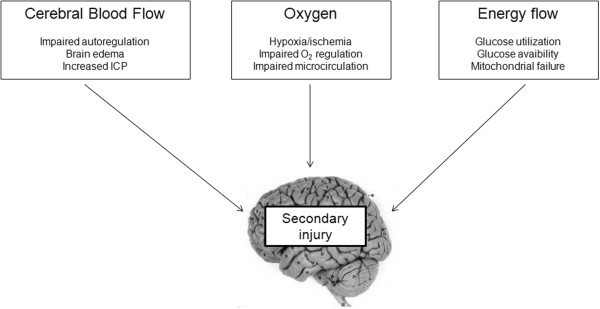
Monitoring and management of intracranial pressure (ICP) and cerebral perfusion pressure (CPP) is a standard of care after traumatic brain injury (TBI). However, the pathophysiology of so-called secondary brain injury, i.e., the cascade of potentially deleterious events that occur in the early phase following initial cerebral insult-after TBI, is complex, involving a subtle interplay between cerebral blood flow (CBF), oxygen delivery and utilization, and supply of main cerebral energy substrates (glucose) to the injured brain. Regulation of this interplay depends on the type of injury and may vary individually and over time. In this setting, patient management can be a challenging task, where standard ICP/CPP monitoring may become insufficient to prevent secondary brain injury. Growing clinical evidence demonstrates that so-called multimodal brain monitoring, including brain tissue oxygen (PbtO2), cerebral microdialysis and transcranial Doppler among others, might help to optimize CBF and the delivery of oxygen/energy substrate at the bedside, thereby improving the management of secondary brain injury. Looking beyond ICP and CPP, and applying a multimodal therapeutic approach for the optimization of CBF, oxygen delivery, and brain energy supply may eventually improve overall care of patients with head injury. This review summarizes some of the important pathophysiological determinants of secondary cerebral damage after TBI and discusses novel approaches to optimize CBF and provide adequate oxygen and energy supply to the injured brain using multimodal brain monitoring.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
