

Multiple major morbidities and increased mortality during long-term follow-up after recovery from thrombotic thrombocytopenic purpura
- PMID: 23838348
- PMCID: PMC3778546
- DOI: 10.1182/blood-2013-04-496752
Multiple major morbidities and increased mortality during long-term follow-up after recovery from thrombotic thrombocytopenic purpura
Abstract
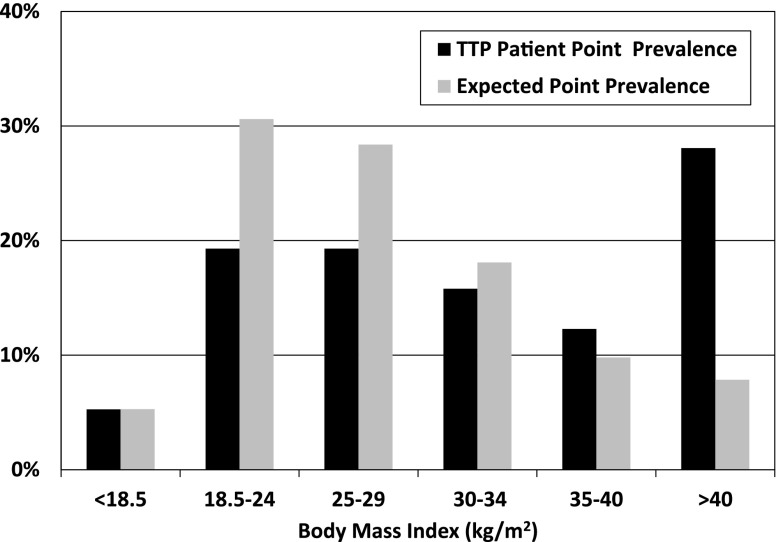
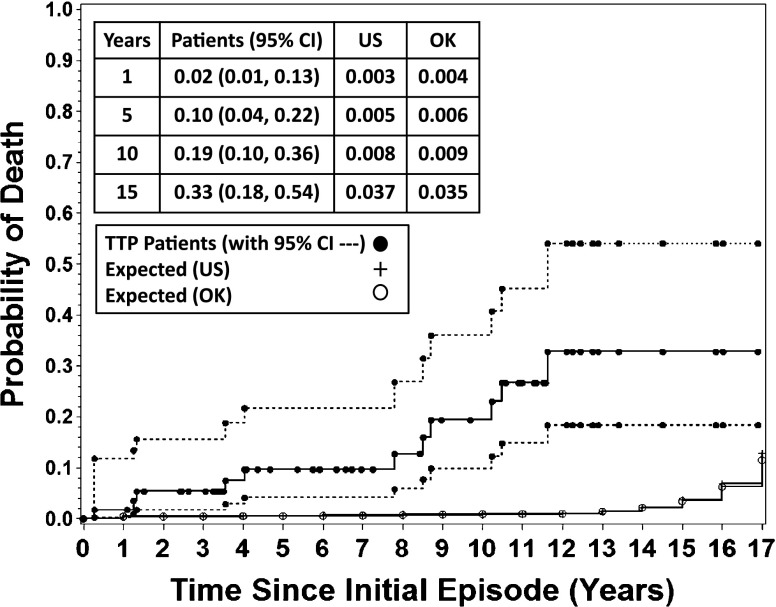
Recovery from acute episodes of thrombotic thrombocytopenic purpura (TTP) appears complete except for minor cognitive abnormalities and risk for relapse. The Oklahoma TTP-HUS (hemolytic uremic syndrome) Registry enrolled 70 consecutive patients from 1995 to 2011 with ADAMTS13 activity <10% at their initial episode; 57 survived, with follow-up through 2012. The prevalence of body mass index (BMI), glomerular filtration rate (GFR), urine albumin/creatinine ratio (ACR), hypertension, major depression, systemic lupus erythematosus (SLE), and risk of death were compared with expected values based on the US reference population. At initial diagnosis, 57 survivors had a median age of 39 years; 45 (79%) were women; 21 (37%) were black; BMI and prevalence of SLE (7%) were greater (P < .001) than expected; prevalence of hypertension (19%; P = .463) was not different. GFR (P = .397) and ACR (P = .793) were not different from expected values. In 2011-2012, prevalence of hypertension (40% vs 23%; P = .013) and major depression (19% vs 6%; P = .005) was greater than expected values. Eleven patients (19%) have died, a proportion greater than expected compared with US and Oklahoma reference populations (P < .05). TTP survivors may have greater risk for poor health and premature death.
Figures


References
-
- George JN. Clinical practice. Thrombotic thrombocytopenic purpura. N Engl J Med. 2006;354(18):1927–1935. - PubMed
-
- Amorosi EL, Ultmann JE. Thrombotic thrombocytopenic purpura: report of 16 cases and review of the literature. Medicine. 1966;45(2):139–160.
-
- Rock GA, Shumak KH, Buskard NA, Blanchette VS, Kelton JG, Nair RC, Spasoff RA Canadian Apheresis Study Group. Comparison of plasma exchange with plasma infusion in the treatment of thrombotic thrombocytopenic purpura. N Engl J Med. 1991;325(6):393–397. - PubMed
-
- Shumak KH, Rock GA, Nair RC Canadian Apheresis Group. Late relapses in patients successfully treated for thrombotic thrombocytopenic purpura. Ann Intern Med. 1995;122(8):569–572. - PubMed
-
- Kremer Hovinga JA, Vesely SK, Terrell DR, Lämmle B, George JN. Survival and relapse in patients with thrombotic thrombocytopenic purpura. Blood. 2010;115(8):1500–1511, quiz 1662. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
