

Geographic variation in cardiovascular procedure use among Medicare fee-for-service vs Medicare Advantage beneficiaries
- PMID: 23839749
- PMCID: PMC4021020
- DOI: 10.1001/jama.2013.7837
Geographic variation in cardiovascular procedure use among Medicare fee-for-service vs Medicare Advantage beneficiaries
Abstract
Importance: Little is known about how different financial incentives between Medicare Advantage and Medicare fee-for-service (FFS) reimbursement structures influence use of cardiovascular procedures.
Objective: To compare regional cardiovascular procedure rates between Medicare Advantage and Medicare FFS beneficiaries.
Design, setting, and participants: Cross-sectional study of Medicare beneficiaries older than 65 years between 2003-2007 comparing rates of coronary angiography, percutaneous coronary intervention (PCI), and coronary artery bypass graft (CABG) surgery across 32 hospital referral regions in 12 states.
Main outcomes and measures: Rates of coronary angiography, PCI, and CABG surgery.
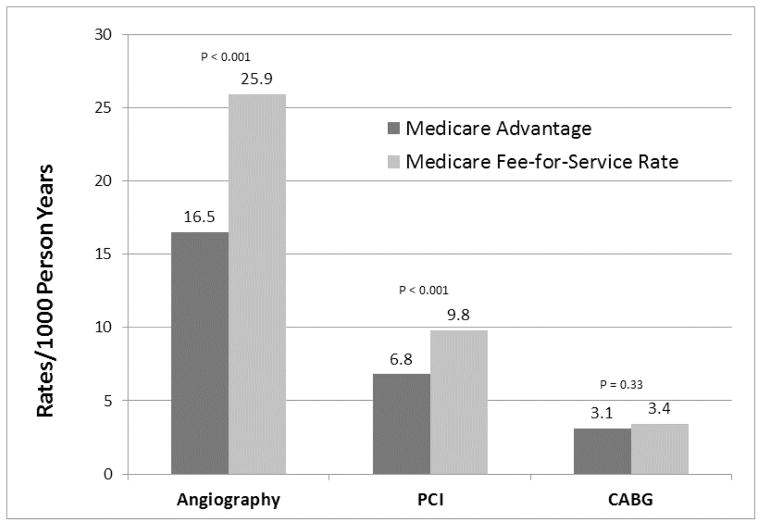
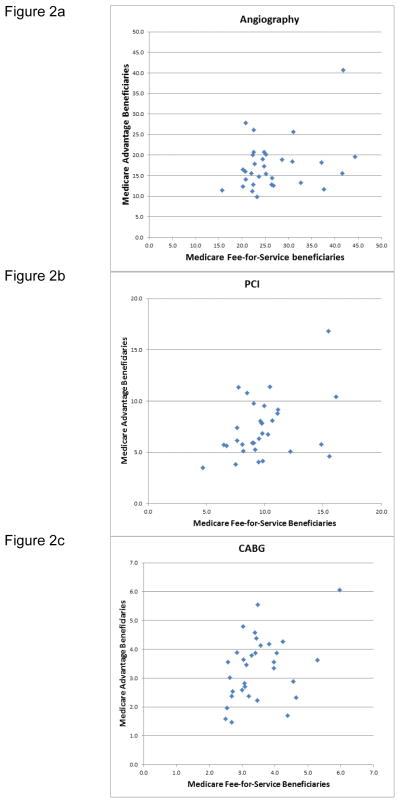
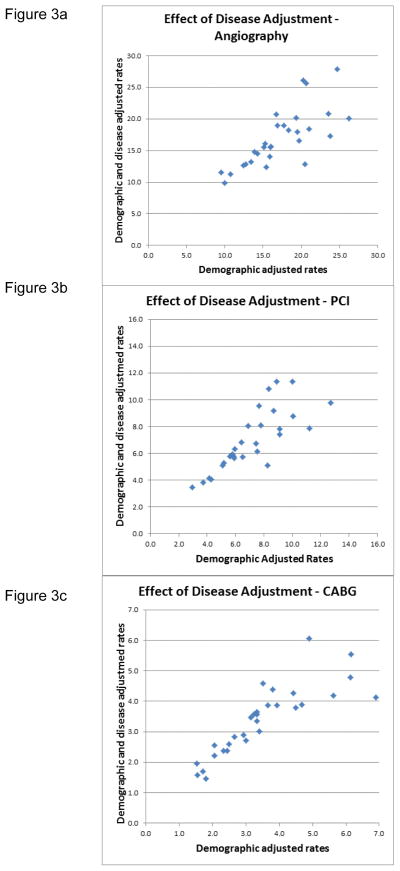
Results: We evaluated a total of 878,339 Medicare Advantage patients and 5,013,650 Medicare FFS patients. Compared with Medicare FFS patients, Medicare Advantage patients had lower age-, sex-, race-, and income-adjusted procedure rates per 1000 person-years for angiography (16.5 [95% CI, 14.8-18.2] vs 25.9 [95% CI, 24.0-27.9]; P < .001) and PCI (6.8 [95% CI, 6.0-7.6] vs 9.8 [95% CI, 9.0-10.6]; P < .001) but similar rates for CABG surgery (3.1 [95% CI, 2.8-3.5] vs 3.4 [95% CI, 3.1-3.7]; P = .33). There were no significant differences between Medicare Advantage and Medicare FFS patients in the rates per 1000 person-years of urgent angiography (3.9 [95% CI, 3.6-4.2] vs 4.3 [95% CI, 4.0-4.6]; P = .24) or PCI (2.4 [95% CI, 2.2-2.7] vs 2.7 [95% CI, 2.5-2.9]; P = .16). Procedure rates varied widely across hospital referral regions among Medicare Advantage and Medicare FFS patients. For angiography, the rates per 1000 person-years ranged from 9.8 to 40.6 for Medicare Advantage beneficiaries and from 15.7 to 44.3 for Medicare FFS beneficiaries. For PCI, the rates ranged from 3.5 to 16.8 for Medicare Advantage and from 4.7 to 16.1 for Medicare FFS. The rates for CABG surgery ranged from 1.5 to 6.1 for Medicare Advantage and from 2.5 to 6.0 for Medicare FFS. Across regions, we found no statistically significant correlation between Medicare Advantage and Medicare FFS beneficiary utilization for angiography (Spearman r = 0.19, P = .29) and modest correlations for PCI (Spearman r = 0.33, P = .06) and CABG surgery (Spearman r = 0.35, P = .05). Among Medicare Advantage beneficiaries, adjustment for additional cardiac risk factors had little influence on procedure rates.
Conclusions and relevance: Although Medicare beneficiaries enrolled in capitated Medicare Advantage programs had lower angiography and PCI procedure rates than those enrolled in Medicare FFS, the degree of geographic variation in procedure rates was substantial among Medicare Advantage beneficiaries and was similar in magnitude to that observed among Medicare FFS beneficiaries.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures
Comment in
-
Variations in health care, patient preferences, and high-quality decision making.JAMA. 2013 Jul 10;310(2):151-2. doi: 10.1001/jama.2013.7835. JAMA. 2013. PMID: 23839747 Free PMC article. No abstract available.
-
Prevalence and extent of obstructive coronary artery disease among patients undergoing elective coronary catheterization in New York State and Ontario.JAMA. 2013 Jul 10;310(2):163-9. doi: 10.1001/jama.2013.7834. JAMA. 2013. PMID: 23839750
References
-
- Heidenreich PA, Trogdon JG, Khavjou OA, et al. Forecasting the Future of Cardiovascular Disease in the United States. Circulation. 2011;123:933–944. - PubMed
-
- Matlock DD, Lucas FL, Malenka D, et al. Regional variation in the use of implantable cardioverter-defibrillators for primary prevention: results from the National Cardiovascular Data Registry. Circ Cardiovasc Qual Outcomes. 2011 Jan 1;4(1):114–21. - PubMed
-
- Wennberg DE, Birkmeyer JD, Birkmeyer NJO. The Dartmouth Atlas of Cardiovascular Health Care. Chicago: AHA Press; 1999.
-
- Ko DT, Wang Y, Alter DA, et al. Regional variation in cardiac catheterization appropriateness and baseline risk after acute myocardial infarction. J Am Col Cardiol. 2008;51:716–723. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
