

Epidemiology of pyrazinamide-resistant tuberculosis in the United States, 1999-2009
- PMID: 23840002
- PMCID: PMC4578633
- DOI: 10.1093/cid/cit452
Epidemiology of pyrazinamide-resistant tuberculosis in the United States, 1999-2009
Abstract
Background: Pyrazinamide (PZA) is essential in tuberculosis treatment. We describe the prevalence, trends, and predictors of PZA resistance in Mycobacterium tuberculosis complex (MTBC) in the United States.
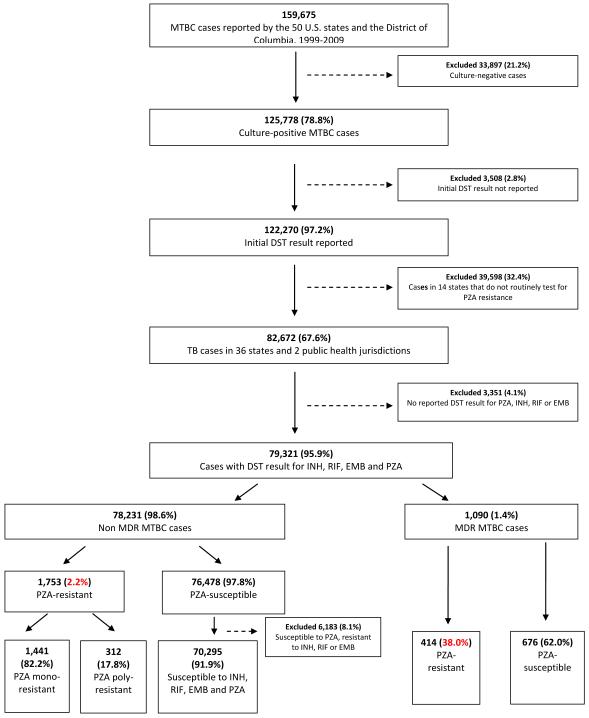
Methods: We analyzed culture-positive MTBC cases with reported drug susceptibility tests for PZA in 38 jurisdictions routinely testing for PZA susceptibility from 1999 to 2009. National Tuberculosis Genotyping Service data for 2004-2009 were used to distinguish M. tuberculosis from Mycobacterium bovis and determine phylogenetic lineage.
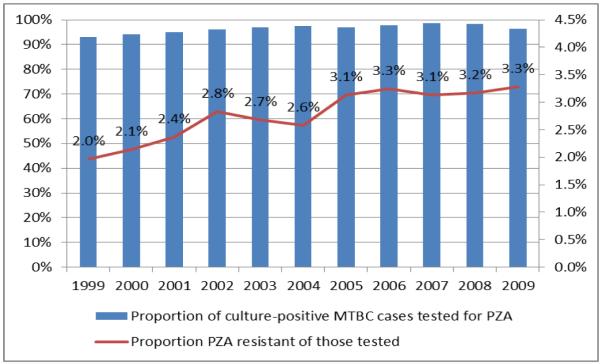
Results: Overall 2.7% (2167/79 321) of MTBC cases had PZA resistance, increasing annually from 2.0% to 3.3% during 1999-2009 (P < .001), largely because of an increase in PZA monoresistance. PZA-monoresistant MTBC (vs drug-susceptible) was associated with an age of 0-24 years (adjusted prevalence ratio [aPR],1.50; 95% confidence interval [CI], 1.31-1.71), Hispanic ethnicity (aPR, 3.52; 95% CI, 2.96-4.18), human immunodeficiency virus infection (aPR, 1.43; 95% CI, 1.15-1.77), extrapulmonary disease (aPR, 3.02; 95% CI, 2.60-3.52), and normal chest radiograph (aPR, 1.88; 95% CI, 1.63-2.16) and was inversely associated with Asian (aPR, 0.59; 95% CI, .47-.73) and black (aPR, 0.37; 95% CI, .29-.49) race. Among multidrug-resistant (MDR) cases, 38.0% were PZA-resistant; PZA resistance in MDR MTBC was associated with female sex (aPR, 1.25; 95% CI, 1.08-1.46) and previous tuberculosis diagnosis (aPR, 1.37; 95% CI, 1.16-1.62). Of 28 080 cases with genotyping data, 925 (3.3%) had PZA resistance; 465 of 925 (50.3%) were M. bovis. In non-MDR M. tuberculosis cases, PZA resistance was higher in the Indo-Oceanic than the East Asian lineage (2.2% vs 0.9%, respectively; aPR, 2.26; 95% CI, 1.53-3.36), but in MDR cases it was lower in the Indo-Oceanic lineage (22.0% vs 43.4%, respectively; aPR, 0.54; 95% CI, .32-.90).
Conclusions: Specific human and mycobacterial characteristics were associated with PZA-resistant MTBC, reflecting both specific subgroups of the population and phylogenetic lineages of the mycobacteria.
Keywords: drug resistance; epidemiology; pyrazinamide; tuberculosis.
Figures




Comment in
-
Next-generation sequencing for identifying pyrazinamide resistance in Mycobacterium tuberculosis.Clin Infect Dis. 2014 Mar;58(6):903-4. doi: 10.1093/cid/cit811. Epub 2013 Dec 12. Clin Infect Dis. 2014. PMID: 24336821 No abstract available.
References
-
- Francis J. Curry National Tuberculosis Center and California Department of Public Health. Drug-Resistant Tuberculosis: A Survival Guide for Clinicians. (2nd) 2008
-
- World Health Organization . Guidelines for the programmatic management of drug-resistant tuberculosis. Geneva, Switzerland: 2011. 2011 update. - PubMed
-
- The U.S. Centers for Disease Control and Prevention Treatment of tuberculosis. Morbidity and mortality weekly report Recommendations and reports. 2003;52(RR-11):1–77. - PubMed
-
- Zhang Y, Mitchison D. The curious characteristics of pyrazinamide: a review. The international journal of tuberculosis and lung disease. 2003;7(1):6–21. - PubMed
-
- Mitchison DA. Role of individual drugs in the chemotherapy of tuberculosis. The international journal of tuberculosis and lung disease. 2000;4(9):796–806. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
