

Clinical and pathological differences between serum immunoglobulin G4-positive and -negative type 1 autoimmune pancreatitis
- PMID: 23840149
- PMCID: PMC3703191
- DOI: 10.3748/wjg.v19.i25.4031
Clinical and pathological differences between serum immunoglobulin G4-positive and -negative type 1 autoimmune pancreatitis
Abstract
Aim: To identify clinical and pathological differences between serum immunoglobulin G4 (IgG4)-positive (SIP) and IgG4-negative (SIN) type 1 autoimmune pancreatitis (AIP) in South Korea.
Methods: AIP was diagnosed by the international consensus diagnostic criteria. The medical records and pathology were retrospectively reviewed and IgG4-positive cells were counted in a high power field (HPF). Type I AIP was defined as a high serum level of IgG4 or histological finding. SIN type 1 AIP was defined as a histological evidence of type 1 AIP and a normal serum IgG4 level. The clinical and pathological findings were compared between the two groups. The analysis was performed using Student's t test, Fischer's exact test and Mann-Whitney's U test. A P value of < 0.05 was considered statistically significant. As repeated comparison was made, P values of less than 5% (P < 0.05) were considered significant.
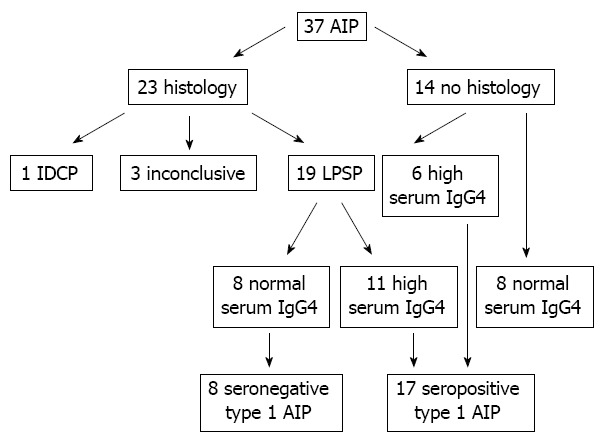
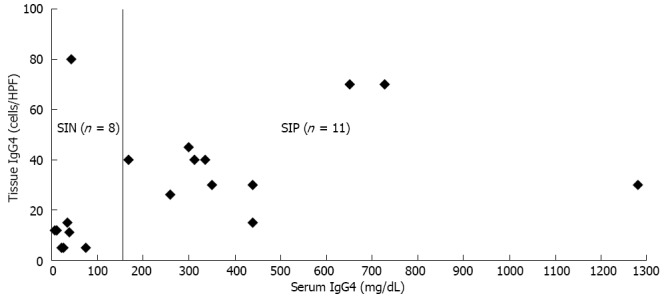
Results: Twenty five patients with definite type 1 AIP (19 histologically and six serologically diagnosed cases) were enrolled. The mean tissue IgG4 concentrations were significantly higher in SIP than SIN group (40 cells per HPF vs 18 cells per HPF, P = 0.02). Among eight SIN patients, the tissue IgG4 concentrations were less than 15 cells per HPF in most of cases, except one. The sensitivity of serum IgG4 was 68% (17 SIP and eight SIN AIP). Other organ involvement was more frequently associated with SIP than SIN AIP (59% vs 26%, P = 0.016). However, the relapse rate and diffuse swelling of the pancreas were not associated with serum IgG4 level. The concentrations of IgG4-positive cells per HPF were higher in SIP than SIN AIP (40 vs 18, P = 0.02).
Conclusion: The sensitivity of serum IgG4 was 68% in type 1 AIP. High serum IgG4 level was associated with other organ involvement and tissue IgG4 concentration but did not affect the relapse rate in type 1 AIP.
Keywords: Autoimmunity; Chronic pancreatitis; Immunoglobulin G4; Immunoglobulin G4-related systemic disease; Lymphoplasmacytic sclerosing pancreatitis.
Figures
Similar articles
-
Increase diagnostic accuracy in differentiating focal type autoimmune pancreatitis from pancreatic cancer with combined serum IgG4 and CA19-9 levels.Pancreatology. 2014 Sep-Oct;14(5):366-72. doi: 10.1016/j.pan.2014.07.010. Epub 2014 Jul 25. Pancreatology. 2014. PMID: 25278306
-
[Clinical observation of isolated immunoglobulin G4-related sclerosing cholangitis and immunoglobulin G4 sclerosing cholangitis combined autoimmune pancreatitis].Zhonghua Gan Zang Bing Za Zhi. 2018 Jun 20;26(6):415-419. doi: 10.3760/cma.j.issn.1007-3418.2018.06.005. Zhonghua Gan Zang Bing Za Zhi. 2018. PMID: 30317753 Chinese.
-
A new diagnostic endoscopic tool for autoimmune pancreatitis.Gastrointest Endosc. 2008 Aug;68(2):358-61. doi: 10.1016/j.gie.2008.02.018. Epub 2008 Jun 2. Gastrointest Endosc. 2008. PMID: 18513718
-
Current Concepts and Diagnosis of IgG4-Related Pancreatitis (Type 1 AIP).Semin Liver Dis. 2016 Aug;36(3):257-73. doi: 10.1055/s-0036-1584318. Epub 2016 Jul 28. Semin Liver Dis. 2016. PMID: 27466795 Review.
-
Diagnosis and classification of autoimmune pancreatitis.Autoimmun Rev. 2014 Apr-May;13(4-5):451-8. doi: 10.1016/j.autrev.2014.01.010. Epub 2014 Jan 12. Autoimmun Rev. 2014. PMID: 24424184 Review.
Cited by
-
Basophils activated via TLR signaling may contribute to pathophysiology of type 1 autoimmune pancreatitis.J Gastroenterol. 2018 Mar;53(3):449-460. doi: 10.1007/s00535-017-1390-6. Epub 2017 Sep 18. J Gastroenterol. 2018. PMID: 28921377 Free PMC article.
-
Challenges for clinicians treating autoimmune pancreatitis: Current perspectives.World J Clin Cases. 2023 Jan 6;11(1):30-46. doi: 10.12998/wjcc.v11.i1.30. World J Clin Cases. 2023. PMID: 36687190 Free PMC article. Review.
-
Concurrent autoimmune pancreatitis and primary biliary cirrhosis: a rare case report and literature review.BMC Gastroenterol. 2014 Jan 10;14:10. doi: 10.1186/1471-230X-14-10. BMC Gastroenterol. 2014. PMID: 24410827 Free PMC article. Review.
-
Serum biomarkers for the differentiation of autoimmune pancreatitis from pancreatic ductal adenocarcinoma.World J Gastrointest Oncol. 2023 Feb 15;15(2):268-275. doi: 10.4251/wjgo.v15.i2.268. World J Gastrointest Oncol. 2023. PMID: 36908319 Free PMC article. Review.
-
The Clinical Utility of Soluble Serum Biomarkers in Autoimmune Pancreatitis: A Systematic Review.Biomedicines. 2022 Jun 26;10(7):1511. doi: 10.3390/biomedicines10071511. Biomedicines. 2022. PMID: 35884816 Free PMC article. Review.
References
-
- Zhang L, Chari S, Smyrk TC, Deshpande V, Klöppel G, Kojima M, Liu X, Longnecker DS, Mino-Kenudson M, Notohara K, et al. Autoimmune pancreatitis (AIP) type 1 and type 2: an international consensus study on histopathologic diagnostic criteria. Pancreas. 2011;40:1172–1179. doi: 10.1097/MPA.0b013e318233bec5. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
