

Rapid Syphilis Tests as Catalysts for Health Systems Strengthening: A Case Study from Peru
- PMID: 23840552
- PMCID: PMC3694115
- DOI: 10.1371/journal.pone.0066905
Rapid Syphilis Tests as Catalysts for Health Systems Strengthening: A Case Study from Peru
Abstract
Objectives: Untreated maternal syphilis leads to adverse pregnancy outcomes. The use of point of care tests (POCT) offers an opportunity to improve screening coverage for syphilis and other aspects of health systems. Our objective is to present the experience of the introduction of POCT for syphilis in Peru and describe how new technology can catalyze health system strengthening.
Methods: The study was implemented from September 2009-November 2010 to assess the feasibility of the use of a POCT for syphilis for screening pregnant women in Lima, Peru. Outcomes measured included access to syphilis screening, treatment coverage, partner treatment, effect on patient flow and service efficiency, acceptability among providers and patients, and sustainability.
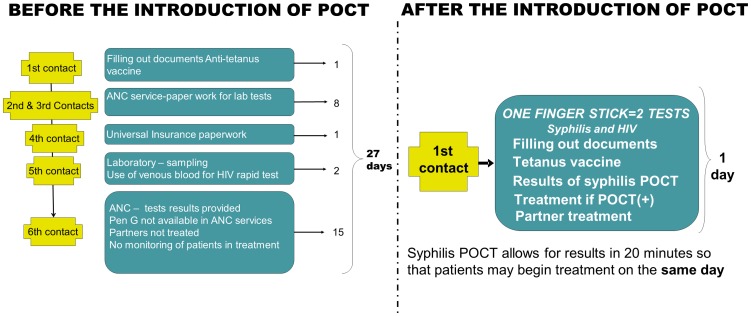
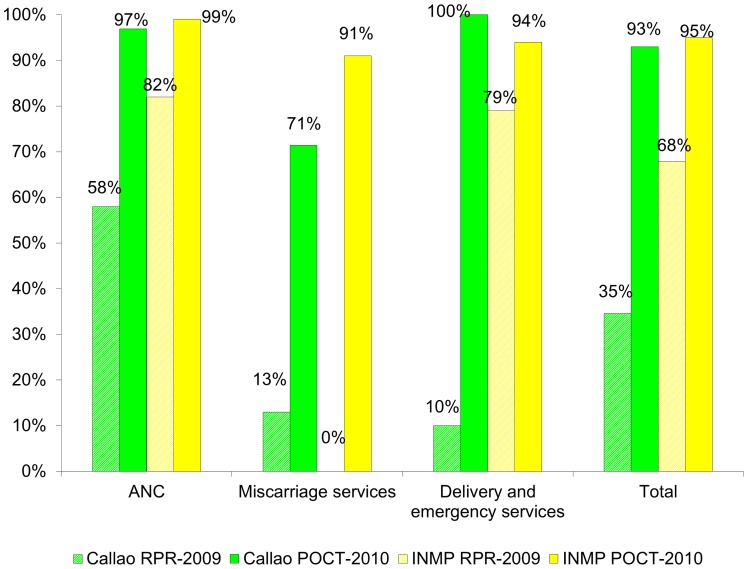
Results: Before the introduction of POCT, a pregnant woman needed 6 visits to the health center in 27 days before she received her syphilis result. We trained 604 health providers and implemented the POCT for syphilis as the "two for one strategy", offering with one finger stick both syphilis and HIV testing. Implementation of the POCT resulted in testing and treatment on the first visit. Screening and treatment coverages for syphilis improved significantly compared with the previous year. Implementation of POCT has been scaled up nationally since the study ended, and coverages for screening, treatment and partner treatment have remained over 92%.
Conclusions: Implementation of POCT for syphilis proved feasible and acceptable, and led to improvement in several aspects of health services. For the process to be effective we highlight the importance of: (1) engaging the authorities; (2) dissipating tensions between providers and identifying champions; (3) training according to the needs; (4) providing monitoring, supervision, support and recognition; (5) sharing results and discussing actions together; (6) consulting and obtaining feedback from users; and (7) integrating with other services such as with rapid HIV testing.
Conflict of interest statement
Figures
Similar articles
-
Integrating HIV, syphilis, malaria and anaemia point-of-care testing (POCT) for antenatal care at dispensaries in western Kenya: discrete-event simulation modelling of operational impact.BMC Public Health. 2019 Dec 3;19(1):1629. doi: 10.1186/s12889-019-7739-4. BMC Public Health. 2019. PMID: 31795999 Free PMC article.
-
Integrated point-of-care testing (POCT) of HIV, syphilis, malaria and anaemia in antenatal clinics in western Kenya: A longitudinal implementation study.PLoS One. 2018 Jul 20;13(7):e0198784. doi: 10.1371/journal.pone.0198784. eCollection 2018. PLoS One. 2018. PMID: 30028852 Free PMC article.
-
The impact of antenatal syphilis point of care testing on pregnancy outcomes: A systematic review.PLoS One. 2021 Mar 25;16(3):e0247649. doi: 10.1371/journal.pone.0247649. eCollection 2021. PLoS One. 2021. PMID: 33765040 Free PMC article.
-
Rollout of rapid point of care tests for antenatal syphilis screening in Ghana: healthcare provider perspectives and experiences.BMC Health Serv Res. 2018 Feb 20;18(1):130. doi: 10.1186/s12913-018-2935-y. BMC Health Serv Res. 2018. PMID: 29458363 Free PMC article.
-
Screening for syphilis infection in pregnant women: evidence for the U.S. Preventive Services Task Force reaffirmation recommendation statement.Ann Intern Med. 2009 May 19;150(10):710-6. doi: 10.7326/0003-4819-150-10-200905190-00009. Ann Intern Med. 2009. PMID: 19451578 Review.
Cited by
-
Point of care diagnostics for sexually transmitted infections: perspectives and advances.Expert Rev Anti Infect Ther. 2014 Jun;12(6):657-72. doi: 10.1586/14787210.2014.880651. Epub 2014 Feb 3. Expert Rev Anti Infect Ther. 2014. PMID: 24484215 Free PMC article. Review.
-
Scaling Down to Scale Up: A Health Economic Analysis of Integrating Point-of-Care Syphilis Testing into Antenatal Care in Zambia during Pilot and National Rollout Implementation.PLoS One. 2015 May 13;10(5):e0125675. doi: 10.1371/journal.pone.0125675. eCollection 2015. PLoS One. 2015. PMID: 25970443 Free PMC article.
-
HIV and syphilis testing preferences among men who have sex with men and among transgender women in Lima, Peru.PLoS One. 2018 Oct 29;13(10):e0206204. doi: 10.1371/journal.pone.0206204. eCollection 2018. PLoS One. 2018. PMID: 30372465 Free PMC article.
-
Sociodemographic and clinical characteristics associated with maternal and congenital syphilis - A prospective study in Peru.Int J Infect Dis. 2024 Jun;143:107041. doi: 10.1016/j.ijid.2024.107041. Epub 2024 Apr 5. Int J Infect Dis. 2024. PMID: 38583824 Free PMC article.
-
Cost-effectiveness of HIV and syphilis antenatal screening: a modelling study.Sex Transm Infect. 2016 Aug;92(5):340-6. doi: 10.1136/sextrans-2015-052367. Epub 2016 Feb 26. Sex Transm Infect. 2016. PMID: 26920867 Free PMC article.
References
-
- Hawkes S, Matin N, Broutet N, Low N (2011) Effectiveness of interventions to improve screening for syphilis in pregnancy: a systematic review and meta-analysis. Lancet Infect Dis 11: 684–691. - PubMed
-
- Watson-Jones D, Gumodoka B, Weiss H, Changalucha J, Todd J, et al. (2002) Syphilis in pregnancy in Tanzania. II. The effectiveness of antenatal syphilis screening and single-dose benzathine penicillin treatment for the prevention of adverse pregnancy outcome. J Infect Dis. 186: 948–957. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
