

Guillain-Barré Syndrome, Influenza Vaccination, and Antecedent Respiratory and Gastrointestinal Infections: A Case-Centered Analysis in the Vaccine Safety Datalink, 2009-2011
- PMID: 23840621
- PMCID: PMC3694016
- DOI: 10.1371/journal.pone.0067185
Guillain-Barré Syndrome, Influenza Vaccination, and Antecedent Respiratory and Gastrointestinal Infections: A Case-Centered Analysis in the Vaccine Safety Datalink, 2009-2011
Abstract
Background: Guillain-Barré Syndrome (GBS) can be triggered by gastrointestinal or respiratory infections, including influenza. During the 2009 influenza A (H1N1) pandemic in the United States, monovalent inactivated influenza vaccine (MIV) availability coincided with high rates of wildtype influenza infections. Several prior studies suggested an elevated GBS risk following MIV, but adjustment for antecedent infection was limited.
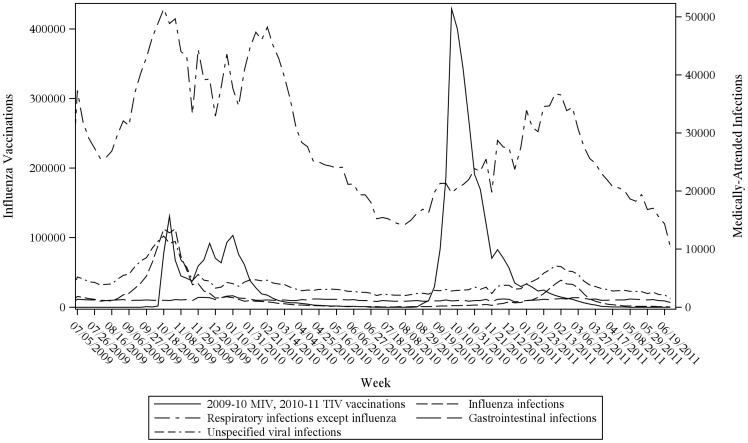
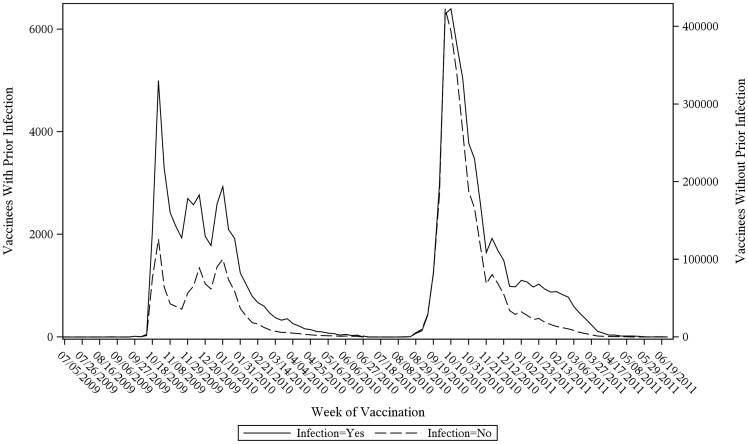
Methods: We identified patients enrolled in health plans participating in the Vaccine Safety Datalink and diagnosed with GBS from July 2009 through June 2011. Medical records of GBS cases with 2009-10 MIV, 2010-11 trivalent inactivated influenza vaccine (TIV), and/or a medically-attended respiratory or gastrointestinal infection in the 1 through 141 days prior to GBS diagnosis were reviewed and classified according to Brighton Collaboration criteria for diagnostic certainty. Using a case-centered design, logistic regression models adjusted for patient-level time-varying sources of confounding, including seasonal vaccinations and infections in GBS cases and population-level controls.
Results: Eighteen confirmed GBS cases received vaccination in the 6 weeks preceding onset, among 1.27 million 2009-10 MIV recipients and 2.80 million 2010-11 TIV recipients. Forty-four confirmed GBS cases had infection in the 6 weeks preceding onset, among 3.77 million patients diagnosed with medically-attended infection. The observed-versus-expected odds that 2009-10 MIV/2010-11 TIV was received in the 6 weeks preceding GBS onset was odds ratio = 1.54, 95% confidence interval (CI), 0.59-3.99; risk difference = 0.93 per million doses, 95% CI, -0.71-5.16. The association between GBS and medically-attended infection was: odds ratio = 7.73, 95% CI, 3.60-16.61; risk difference = 11.62 per million infected patients, 95% CI, 4.49-26.94. These findings were consistent in sensitivity analyses using alternative infection definitions and risk intervals for prior vaccination shorter than 6 weeks.
Conclusions: After adjusting for antecedent infections, we found no evidence for an elevated GBS risk following 2009-10 MIV/2010-11 TIV influenza vaccines. However, the association between GBS and antecedent infection was strongly elevated.
Conflict of interest statement
Figures
References
-
- Yuki N, Hartung HP (2012) Guillain-Barré syndrome. N Engl J Med 366: 2294–2304. - PubMed
-
- Jacobs BC, Rothbarth PH, van der Meche FG, Herbrink P, Schmitz PI, et al. (1998) The spectrum of antecedent infections in Guillain-Barré syndrome: a case-control study. Neurology 51: 1110–1115. - PubMed
-
- Koga M, Gilbert M, Li J, Koike S, Takahashi M, et al. (2005) Antecedent infections in Fisher syndrome: a common pathogenesis of molecular mimicry. Neurology 64: 1605–1611. - PubMed
-
- Hughes RA, Cornblath DR (2005) Guillain-Barré syndrome. Lancet 366: 1653–1666. - PubMed
-
- Shui IM, Rett MD, Weintraub E, Marcy M, Amato AA, et al. (2012) Guillain-Barré syndrome incidence in a large United States cohort (2000–2009). Neuroepidemiology 39: 109–115. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
