

An atypical age-specific pattern of hepatocellular carcinoma in Peru: a threat for Andean populations
- PMID: 23840771
- PMCID: PMC3695993
- DOI: 10.1371/journal.pone.0067756
An atypical age-specific pattern of hepatocellular carcinoma in Peru: a threat for Andean populations
Abstract
Background: In South America, the highest incidence of primary liver cancer is observed in Peru. However, national estimations on hepatocellular carcinoma incidence and mortality are approximated using aggregated data from surrounding countries. Thus, there is a lack of tangible information from Peru that impairs an accurate description of the local incidence, presentation, and outcomes of hepatocellular carcinoma. The present study attempts to fill this gap and assesses the clinical epidemiology of hepatocellular carcinoma in this country.
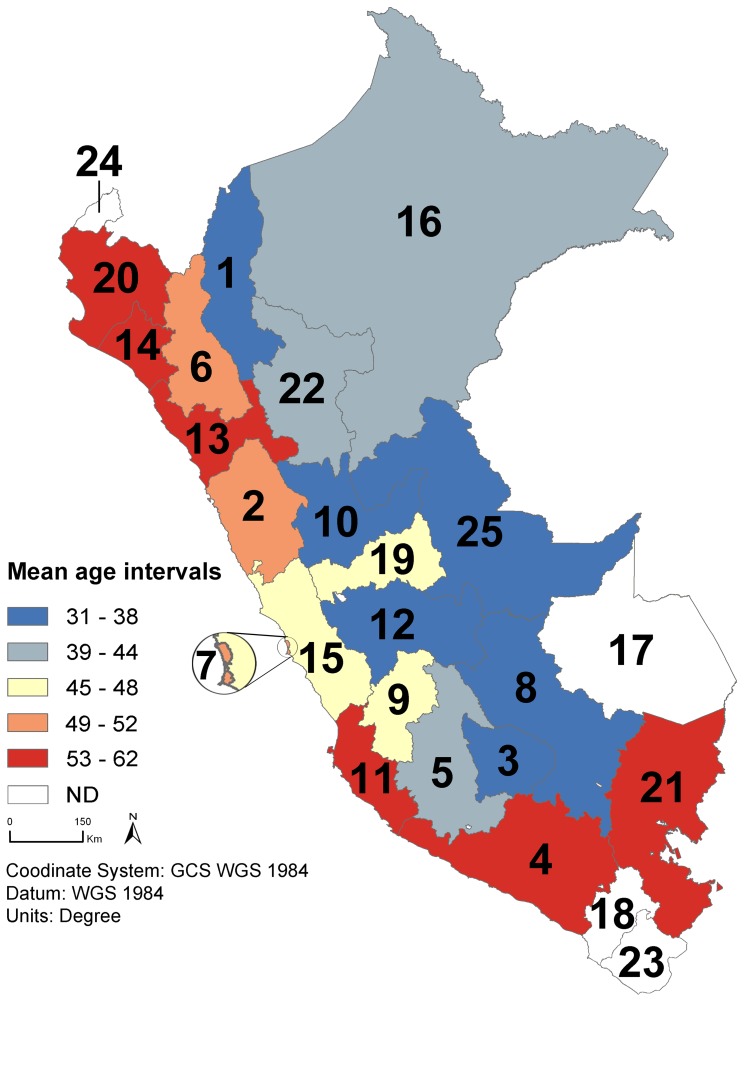
Methods: A retrospective cohort study was conducted by analysing the medical charts of 1,541 patients with hepatocellular carcinoma admitted between 1997 and 2010 at the Peruvian national institute for cancer. The medical records including liver function, serologic status, and tumor pathology and stage were monitored. Statistical analyses were performed in order to characterize tumor presentation according to demographic features, risk factors, and regional origin.
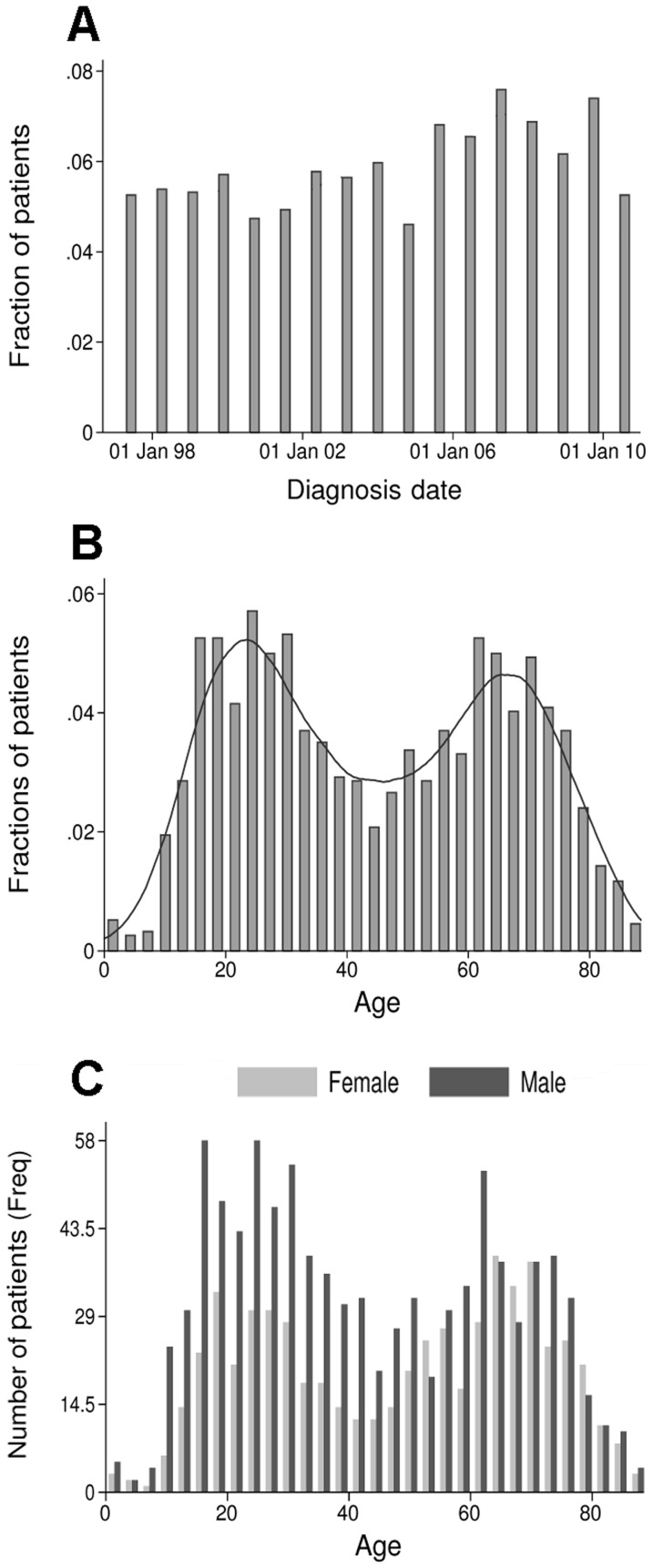
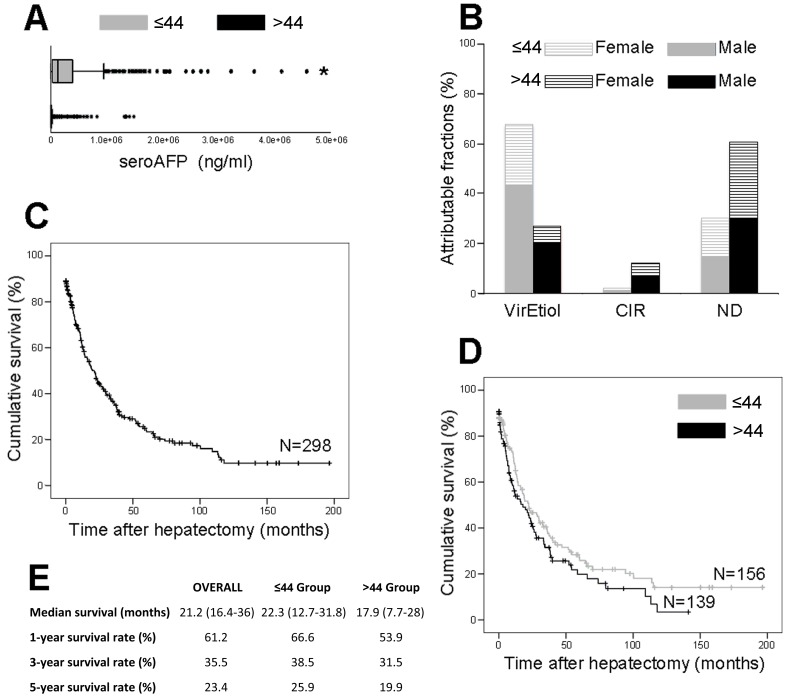
Results: Surprisingly, the age distribution of the patient population displayed bimodality corresponding to two distinct age-based subpopulations. While an older group was in keeping with the age range observed for hepatocellular carcinoma around the world, a younger population displayed an abnormally juvenile mean age of 25.5 years old. In addition, each subpopulation displayed age-specific pathophysiological and clinical characteristics.
Conclusions: The analysis suggests two different age-specific natural histories of hepatocellular carcinoma in the Peruvian patient population. This otherwise unusual tumor process that is ongoing in younger patients leads to the hypothesis that there may be a Peru-endemic risk factor driving hepatocarcinogenesis in the local population.
Conflict of interest statement
Figures
References
-
- Ferlay J, Shin HR, Bray F, Forman D, Mathers C, et al. (2008) Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int J Cancer 127: 2893–2917. - PubMed
-
- Soerjomataram I, Lortet-Tieulent J, Parkin DM, Ferlay J, Mathers C, et al. (2012) Global burden of cancer in 2008: a systematic analysis of disability-adjusted life-years in 12 world regions. Lancet 380: 1840–1850. - PubMed
-
- El-Serag HB (2011) Hepatocellular carcinoma. N Engl J Med 365: 1118–1127. - PubMed
-
- Forner A, Llovet JM, Bruix J (2012) Hepatocellular carcinoma. Lancet 379: 1245–1255. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
