

Detection of anti-HLA antibodies in maternal blood in the second trimester to identify patients at risk of antibody-mediated maternal anti-fetal rejection and spontaneous preterm delivery
- PMID: 23841577
- PMCID: PMC4154511
- DOI: 10.1111/aji.12141
Detection of anti-HLA antibodies in maternal blood in the second trimester to identify patients at risk of antibody-mediated maternal anti-fetal rejection and spontaneous preterm delivery
Abstract
Problem: Maternal anti-fetal rejection is a mechanism of disease in spontaneous preterm labor. The objective of this study was to determine whether the presence of human leukocyte antigen (HLA) panel-reactive antibodies (PRA) during the second trimester increases the risk of spontaneous preterm delivery.
Methods of study: This longitudinal case-control study included pregnant women with spontaneous preterm deliveries (n = 310) and control patients with normal term pregnancies (n = 620), matched for maternal age and gravidity. Maternal plasma samples obtained at 14-16, 16-20, 20-24, and 24-28 weeks of gestation were analyzed for HLA class I and class II PRA positivity using flow cytometry. The fetal HLA genotype and maternal HLA alloantibody epitope were determined for a subset of patients with positive HLA PRA.
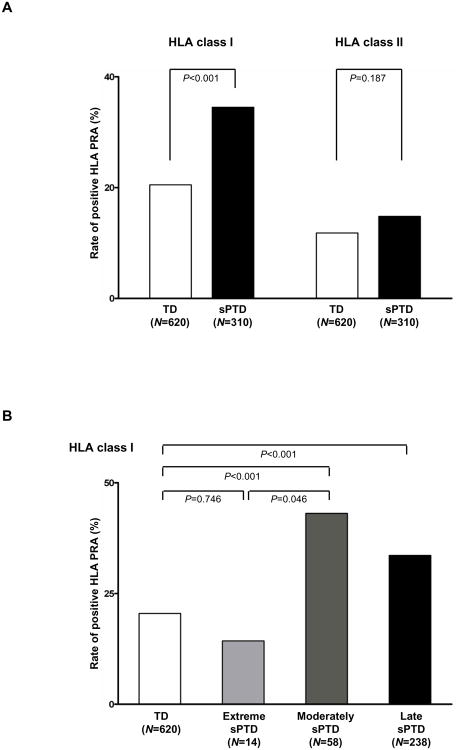
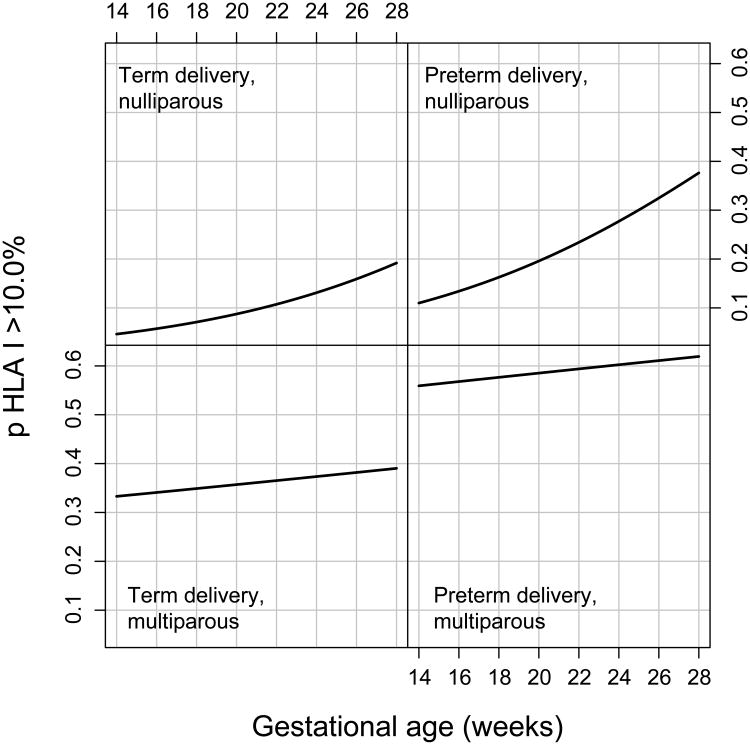
Results: (i) Patients with spontaneous preterm delivery were more likely to exhibit HLA class I (adjusted OR = 2.54, P < 0.0001) and class II (adjusted OR = 1.98, P = 0.002) PRA positivity than those delivering at term; (ii) HLA class I PRA positivity for patients with spontaneous preterm delivery between 28 and 34 weeks (adjusted OR = 2.88; P = 0.001) and after 34 weeks of gestation (adjusted OR = 2.53; P < 0.0001) was higher than for those delivering at term; (iii) HLA class II PRA positivity for patients with spontaneous preterm delivery after 34 weeks of gestation was higher than for those delivering at term (adjusted OR = 2.04; P = 0.002); (iv) multiparous women were at a higher risk for HLA class I PRA positivity than nulliparous women (adjusted OR = 0.097, P < 0.0001 for nulliparity); (v) nulliparous women had a higher rate of HLA class I PRA positivity with advancing gestational age (P = 0.001); and (vi) 78% of women whose fetuses were genotyped had alloantibodies specific against fetal HLA class I antigens.
Conclusion: Pregnant women with positive HLA class I or class II PRA during the second trimester are at an increased risk of spontaneous preterm delivery due to antibody-mediated maternal anti-fetal rejection.
Keywords: Flow cytometry; preterm birth; rejection; transplantation.
Published 2013. This article is a US Government work and is in the public domain in the USA.
Figures
References
-
- Martin JA, Hamilton BE, Sutton PD, Ventura SJ, Menacker F, Kirmeyer S, Munson ML. Births: final data for 2005. National vital statistics reports : from the Centers for Disease Control and Prevention, National Center for Health Statistics, National Vital Statistics System. 2007;56:1–103. - PubMed
-
- Goldenberg RL, McClure EM. The Epidemiology of Preterm Birth. In: Berghella V, editor. Preterm Birth Prevention & Management. Wiley-Blackwell; 2010.
-
- Steer P. The epidemiology of preterm labour. BJOG : an international journal of obstetrics and gynaecology. 2005;112 Suppl 1:1–3. - PubMed
-
- Chang HH, Larson J, Blencowe H, Spong CY, Howson CP, Cairns-Smith S, Lackritz EM, Lee SK, Mason E, Serazin AC, Walani S, Simpson JL, Lawn JE. Preventing preterm births: analysis of trends and potential reductions with interventions in 39 countries with very high human development index. Lancet. 2013;381:223–234. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
