

Diffuse large B-cell lymphoma (Richter syndrome) in patients with chronic lymphocytic leukaemia (CLL): a cohort study of newly diagnosed patients
- PMID: 23841899
- PMCID: PMC4098845
- DOI: 10.1111/bjh.12458
Diffuse large B-cell lymphoma (Richter syndrome) in patients with chronic lymphocytic leukaemia (CLL): a cohort study of newly diagnosed patients
Abstract
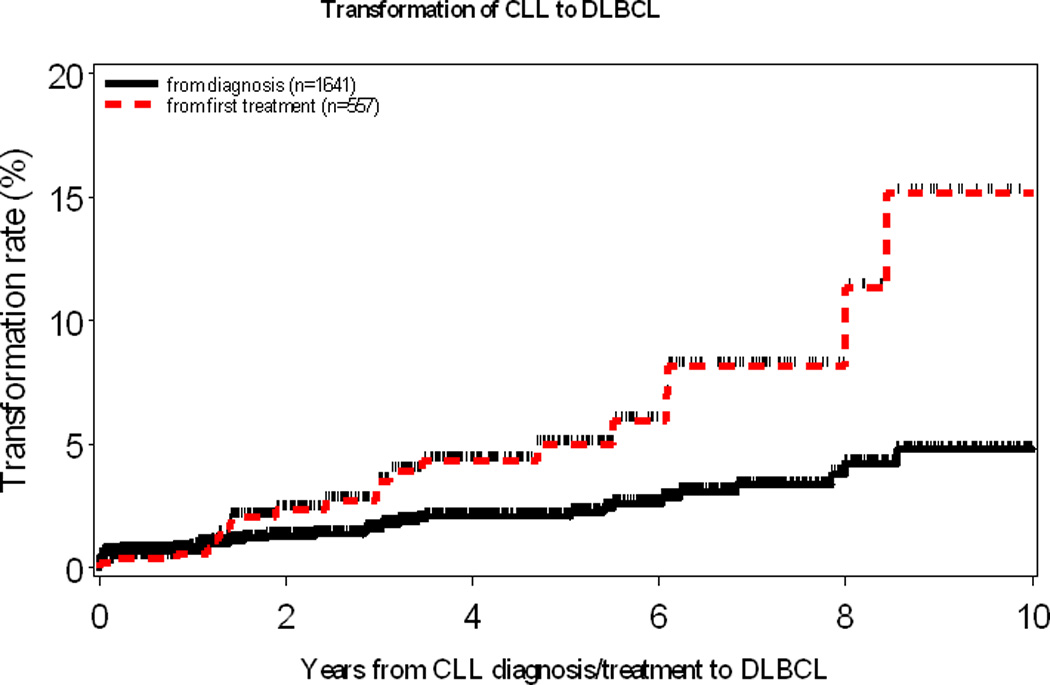
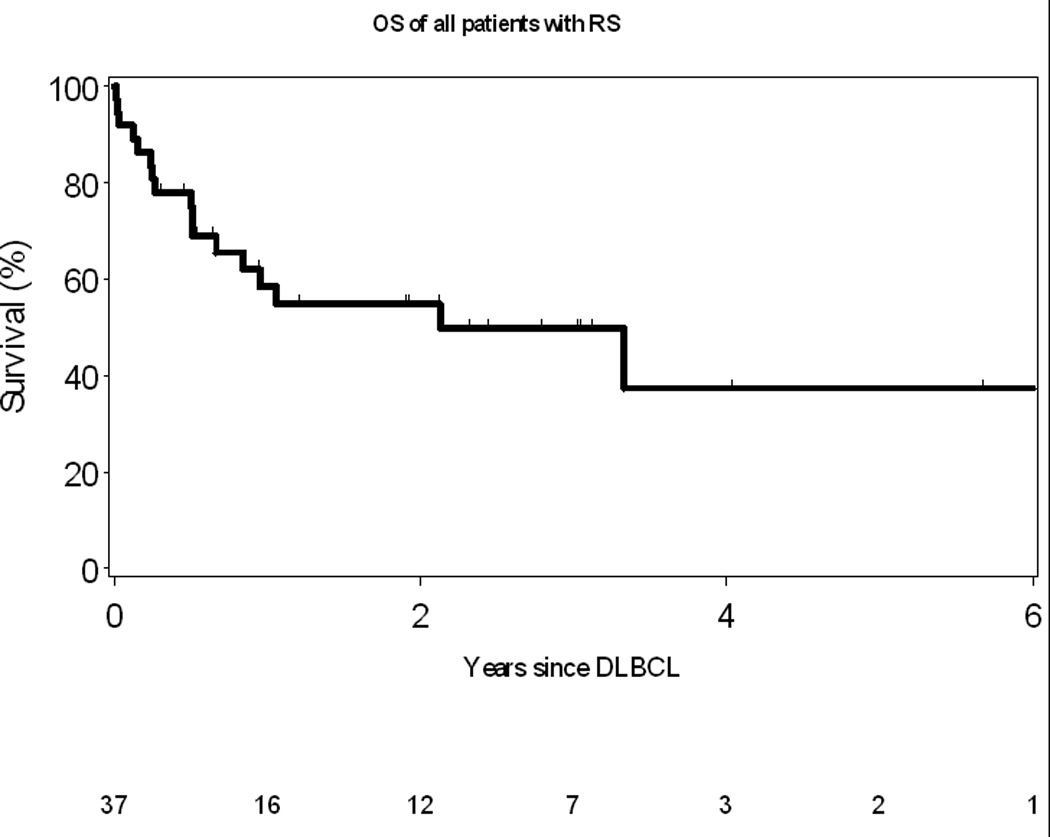
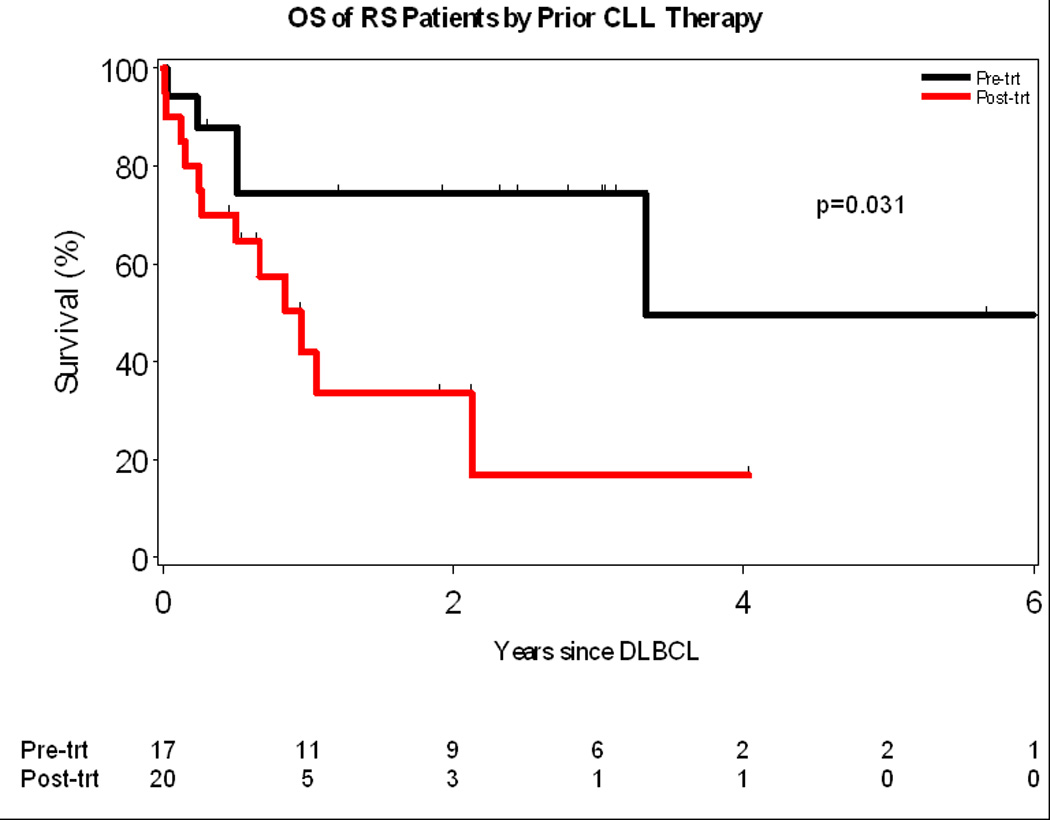
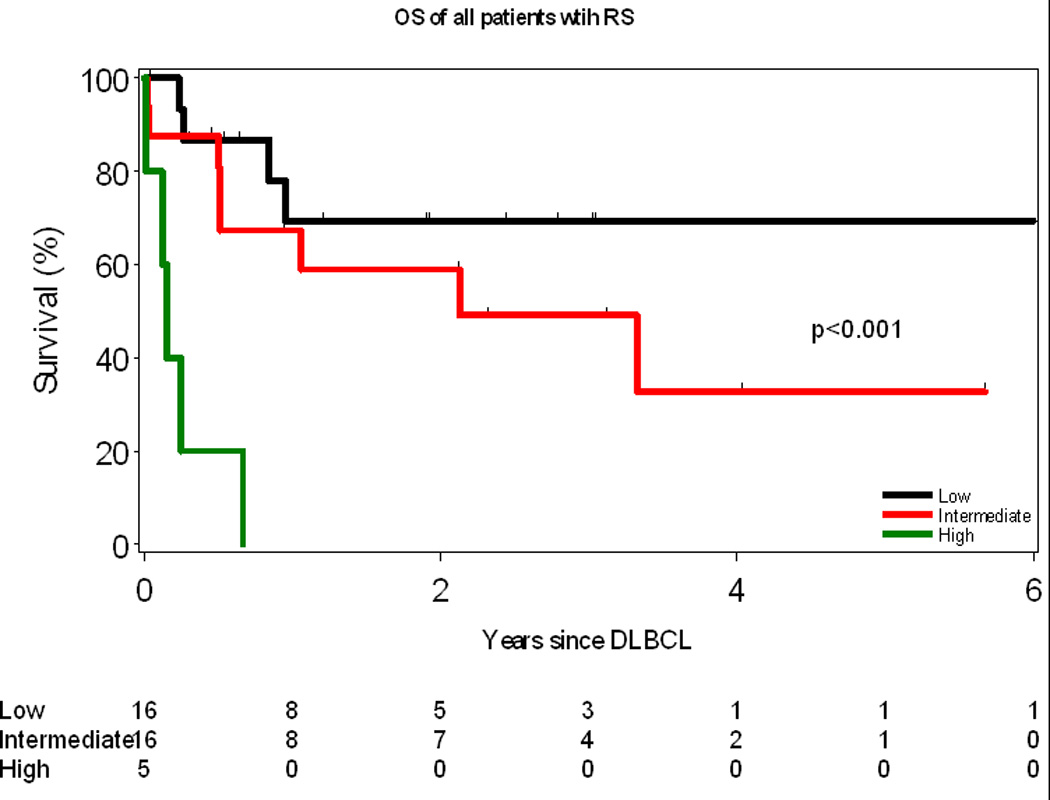
Nearly all information about patients with chronic lymphocytic leukaemia (CLL) who develop diffuse large B-cell lymphoma [Richter syndrome (RS)] is derived from retrospective case series or patients treated on clinical trials. We used the Mayo Clinic CLL Database to identify patients with newly diagnosed CLL between January 2000 and July 2011. Individuals who developed biopsy-proven RS during follow-up were identified. After a median follow-up of 4 years, 37/1641 (2·3%) CLL patients developed RS. The rate of RS was approximately 0·5%/year. Risk of RS was associated with advanced Rai stage at diagnosis (P < 0·001), high-risk genetic abnormalitites on fluorescence in situ hybridization (P < 0·0001), unmutated IGHV (P = 0·003), and expression of ZAP70 (P = 0·02) and CD38 (P = 0·001). The rate of RS doubled in patients after treatment for CLL (1%/year). Stereotyped B-cell receptors (odds-ratio = 4·2; P = 0·01) but not IGHV4-39 family usage was associated with increased risk of RS. Treatment with combination of purine analogues and alkylating agents increased the risk of RS three-fold (odds-ratio = 3·26, P = 0·0003). Median survival after RS diagnosis was 2·1 years. The RS prognosis score stratified patients into three risk groups with median survivals of 0·5 years, 2·1 years and not reached. Both underlying characteristics of the CLL clone and subsequent CLL therapy influence the risk of RS. Survival after RS remains poor and new therapies are needed.
Keywords: Richter syndrome survival score; aggressive lymphoma; purine analogues; stem cell transplantation; transformation.
© 2013 John Wiley & Sons Ltd.
Figures
References
-
- Armitage JO, Dick FR, Corder MP. Diffuse histiocytic lymphoma complicating chronic lymphocytic leukemia. Cancer. 1978;41:422–427. - PubMed
-
- Aydin S, Rossi D, Bergui L, D'Arena G, Ferrero E, Bonello L, Omede P, Novero D, Morabito F, Carbone A, Gaidano G, Malavasi F, Deaglio S. CD38 gene polymorphism and chronic lymphocytic leukemia: a role in transformation to Richter syndrome? Blood. 2008;111:5646–5653. - PubMed
-
- Catovsky D, Richards S, Matutes E, Oscier D, Dyer MJ, Bezares RF, Pettitt AR, Hamblin T, Milligan DW, Child JA, Hamilton MS, Dearden CE, Smith AG, Bosanquet AG, Davis Z, Brito-Babapulle V, Else M, Wade R, Hillmen P. Assessment of fludarabine plus cyclophosphamide for patients with chronic lymphocytic leukaemia (the LRF CLL4 Trial): a randomised controlled trial. Lancet. 2007;370:230–239. - PubMed
-
- Cheson BD, Bennett JM, Grever M, Kay N, Keating MJ, O'Brien S, Rai KR. National Cancer Institute-sponsored Working Group guidelines for chronic lymphocytic leukemia: revised guidelines for diagnosis and treatment. Blood. 1996;87:4990–4997. - PubMed
-
- Cwynarski K, van Biezen A, de Wreede L, Stilgenbauer S, Bunjes D, Metzner B, Koza V, Mohty M, Remes K, Russell N, Nagler A, Scholten M, de Witte T, Sureda A, Dreger P. Autologous and Allogeneic Stem-Cell Transplantation for Transformed Chronic Lymphocytic Leukemia (Richter's Syndrome): A Retrospective Analysis From the Chronic Lymphocytic Leukemia Subcommittee of the Chronic Leukemia Working Party and Lymphoma Working Party of the European Group for Blood and Marrow Transplantation. Journal of Clinical Oncology. 2012;30:2211–2217. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
