

Esophageal atresia in newborns: a wide spectrum from the isolated forms to a full VACTERL phenotype?
- PMID: 23842449
- PMCID: PMC3726359
- DOI: 10.1186/1824-7288-39-45
Esophageal atresia in newborns: a wide spectrum from the isolated forms to a full VACTERL phenotype?
Abstract
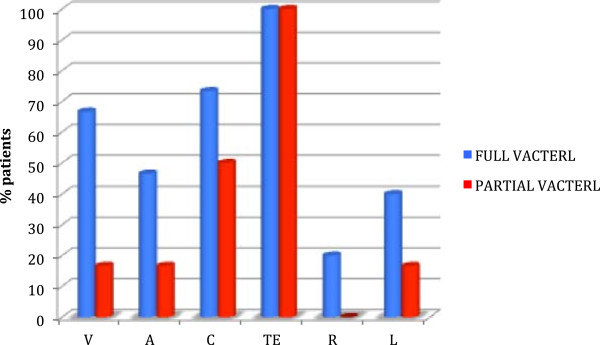
Background: VATER association was first described in 1972 by Quan and Smith as an acronym which identifies a non-random co-occurrence of Vertebral anomalies, Anal atresia, Tracheoesophageal fistula and/or Esophageal atresia, Radial dysplasia. It is even possible to find out Cardiovascular, Renal and Limb anomalies and the acronym VACTERL was adopted, also, embodying Vascular, as single umbilical artery, and external genitalia anomalies.
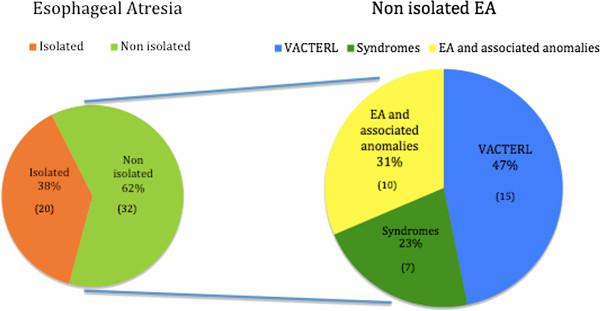
Methods: Data on patients with esophageal atresia (EA) with or without tracheoesophageal fistula (TEF) admitted in the Neonatal Intensive Care Unit (NICU) between January 2003 and January 2013 were evaluated for the contingent occurrence of typical VACTERL anomalies (VACTERL-type) and non tipical VACTERL anomalies (non-VACTERL-type). The inclusion criterion was the presence of EA with or without TEF plus two or more of the following additional malformations: vertebral defects, anal atresia, cardiovascular defects, renal anomalies and lower limb deformities, like radial dysplasia.
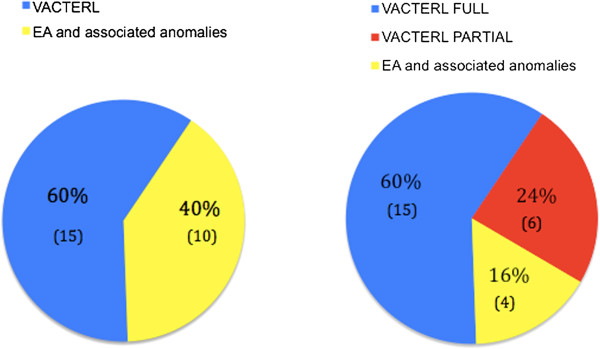
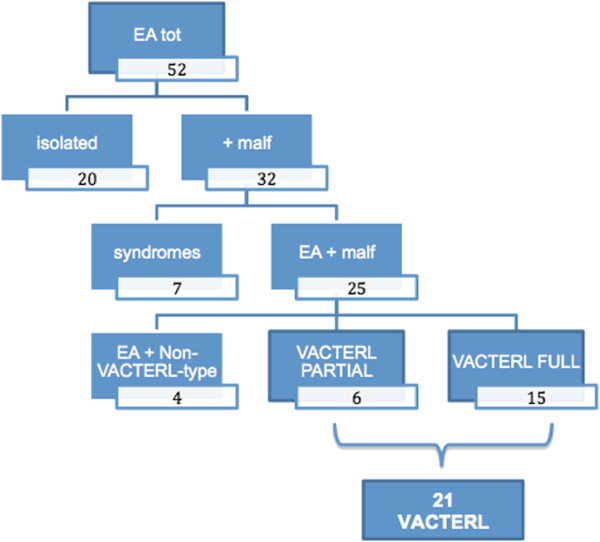
Results: Among 52 patients with EA/TEF, 20 (38,4%) had isolated EA and 7 (21,8%) had a recognized etiology such a syndrome and therefore were excluded. Among 32 infants with EA and associated malformations, 15 (46,8%) had VACTERL association. The most common anomalies were congenital heart defects (73,3%), followed by vertebral anomalies (66,6%). Many patients also had additional non-VACTERL-type defects. Single umbilical artery was the most common one followed by nervous system abnormalities and anomalies of toes. Between the groups of infants with VACTERL type and non-VACTERL-type anomalies, there are several overlapping data regarding both the tipically described spectrum and the most frequently reported non-VACTERL-type malformations. Thus, it is possible to differentiate infants with a full phenotype (VACTERL full phenotype) and patients that do not meet all the criteria mentioned above, but with some homologies with the first group (VACTERL partial phenotype).
Conclusion: The high frequency of non-VACTERL-type anomalies encountered in full and partial phenotype patients would suggest the need for an extension of the clinical criteria for the diagnosis of VACTERL association and also for pre- and post-operative management and follow-up in the short and long term.
Figures
Similar articles
-
VACTERL associations in children undergoing surgery for esophageal atresia and anorectal malformations: Implications for pediatric surgeons.J Pediatr Surg. 2015 Aug;50(8):1245-50. doi: 10.1016/j.jpedsurg.2015.02.049. Epub 2015 Mar 10. J Pediatr Surg. 2015. PMID: 25913268
-
Second study on the recurrence risk of isolated esophageal atresia with or without trachea-esophageal fistula among first-degree relatives: no evidence for increased risk of recurrence of EA/TEF or for malformations of the VATER/VACTERL association spectrum.Birth Defects Res A Clin Mol Teratol. 2013 Dec;97(12):786-91. doi: 10.1002/bdra.23205. Epub 2013 Dec 5. Birth Defects Res A Clin Mol Teratol. 2013. PMID: 24307608
-
Etiological heterogeneity and clinical variability in newborns with esophageal atresia.Ital J Pediatr. 2018 Jan 26;44(1):19. doi: 10.1186/s13052-018-0445-5. Ital J Pediatr. 2018. PMID: 29373986 Free PMC article.
-
VACTERL/VATER Association.Orphanet J Rare Dis. 2011 Aug 16;6:56. doi: 10.1186/1750-1172-6-56. Orphanet J Rare Dis. 2011. PMID: 21846383 Free PMC article. Review.
-
Underlying genetic factors of the VATER/VACTERL association with special emphasis on the "Renal" phenotype.Pediatr Nephrol. 2016 Nov;31(11):2025-33. doi: 10.1007/s00467-016-3335-3. Epub 2016 Feb 8. Pediatr Nephrol. 2016. PMID: 26857713 Free PMC article. Review.
Cited by
-
Review: Hormone Pregnancy Tests Were Teratogenic by the Same Failed Abortion and Hypoxia-Related Mechanism as Misoprostol.Birth Defects Res. 2025 Mar;117(3):e2462. doi: 10.1002/bdr2.2462. Birth Defects Res. 2025. PMID: 40084490 Free PMC article. Review.
-
VACTERL association-type anomalies in a male neonate with a Y-chromosome abnormality.Oxf Med Case Reports. 2015 Jan 10;2015(1):164-6. doi: 10.1093/omcr/omu062. eCollection 2015 Jan. Oxf Med Case Reports. 2015. PMID: 25988067 Free PMC article.
-
Respiratory Morbidity in Children with Repaired Congenital Esophageal Atresia with or without Tracheoesophageal Fistula.Int J Environ Res Public Health. 2017 Sep 27;14(10):1136. doi: 10.3390/ijerph14101136. Int J Environ Res Public Health. 2017. PMID: 28953251 Free PMC article. Review.
-
Is horseshoe lung a component of VACTERL spectrum? Case report and review of literature.Radiol Case Rep. 2022 Mar 8;17(5):1558-1562. doi: 10.1016/j.radcr.2022.02.014. eCollection 2022 May. Radiol Case Rep. 2022. PMID: 35282320 Free PMC article.
-
Developmental basis of trachea-esophageal birth defects.Dev Biol. 2021 Sep;477:85-97. doi: 10.1016/j.ydbio.2021.05.015. Epub 2021 May 21. Dev Biol. 2021. PMID: 34023332 Free PMC article. Review.
References
-
- Quan L, Smith DW. In: The clinical delineation of birth defects. Volume XII. G.I. tract including liver and pancreas. Bergsma D, editor. Baltimore: The Williams and Wilkins company; 1972. The VATER association: vertebral defects, anal atresia, tracheoesophageal fistula with esophageal atresia, radial dysplasia; pp. 75–78.
-
- Hall BD. In: Management of genetic syndromes. Third. Suzanne B, Cassidy MD, Allanson JE, editor. Hoboken, New Jersey: Pubblished by John Wiley & sons Inc.; 2010. VATER/VACTERL association; pp. 871–878.
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
