

Acupuncture-evoked response in somatosensory and prefrontal cortices predicts immediate pain reduction in carpal tunnel syndrome
- PMID: 23843881
- PMCID: PMC3703406
- DOI: 10.1155/2013/795906
Acupuncture-evoked response in somatosensory and prefrontal cortices predicts immediate pain reduction in carpal tunnel syndrome
Abstract
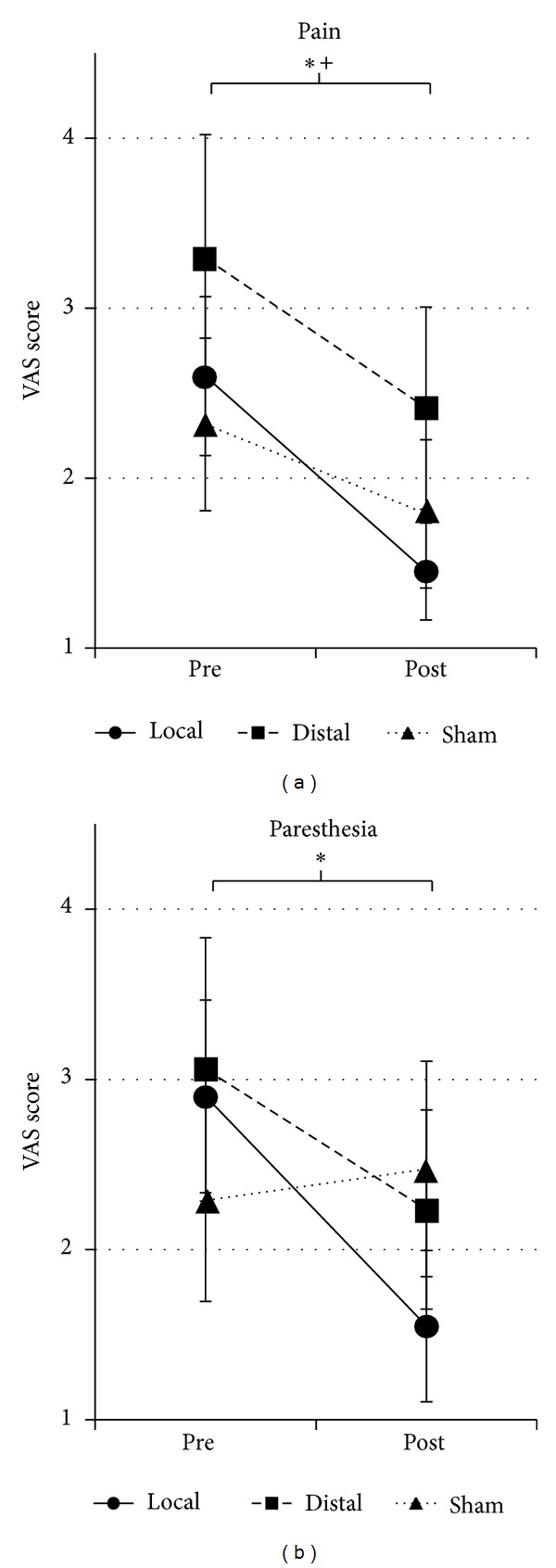
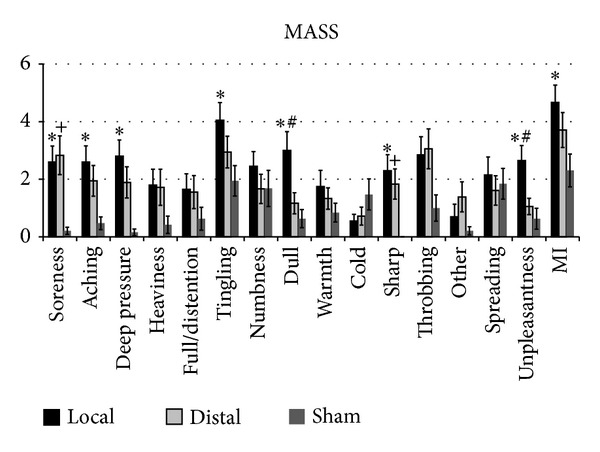
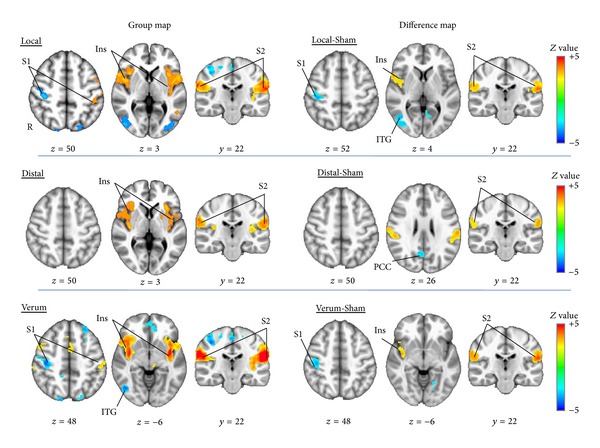
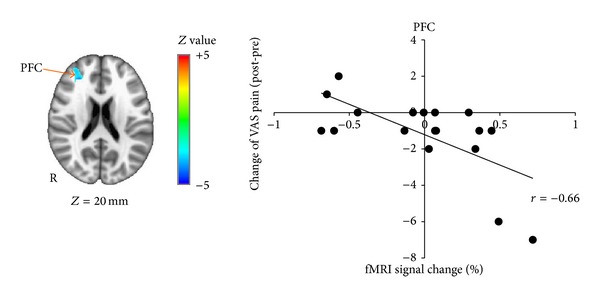
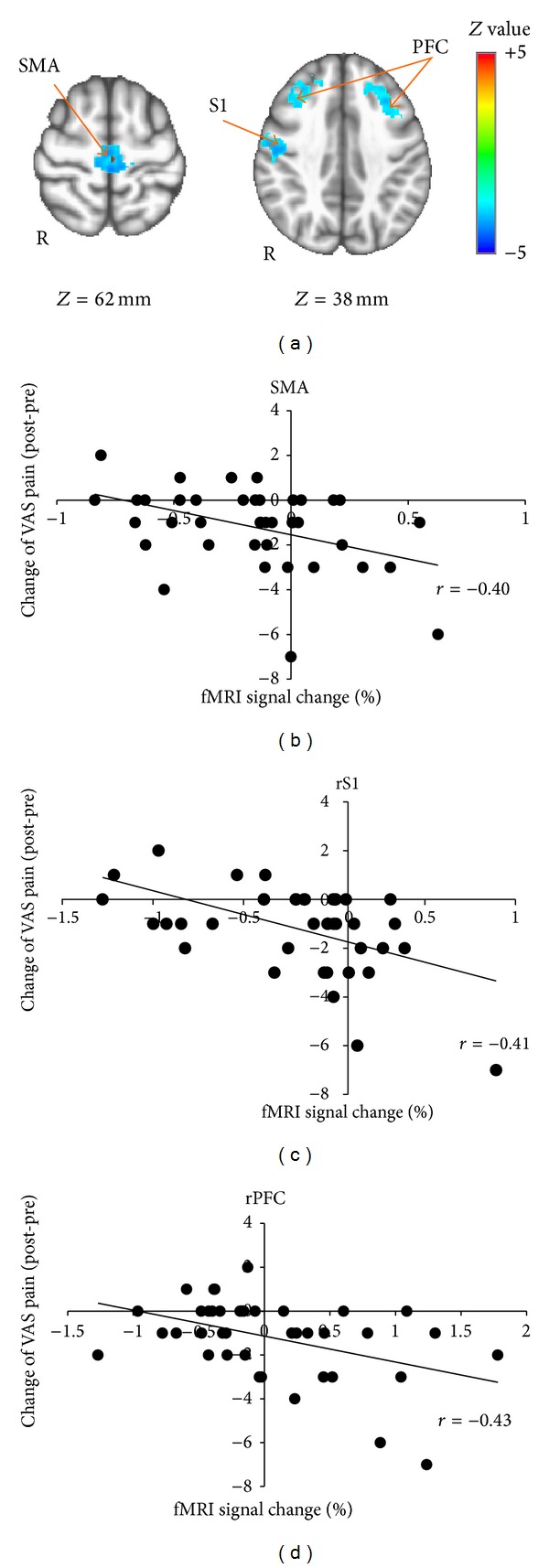
The linkage between brain response to acupuncture and subsequent analgesia remains poorly understood. Our aim was to evaluate this linkage in chronic pain patients with carpal tunnel syndrome (CTS). Brain response to electroacupuncture (EA) was evaluated with functional MRI. Subjects were randomized to 3 groups: (1) EA applied at local acupoints on the affected wrist (PC-7 to TW-5), (2) EA at distal acupoints (contralateral ankle, SP-6 to LV-4), and (3) sham EA at nonacupoint locations on the affected wrist. Symptom ratings were evaluated prior to and following the scan. Subjects in the local and distal groups reported reduced pain. Verum EA produced greater reduction of paresthesia compared to sham. Compared to sham EA, local EA produced greater activation in insula and S2 and greater deactivation in ipsilateral S1, while distal EA produced greater activation in S2 and deactivation in posterior cingulate cortex. Brain response to distal EA in prefrontal cortex (PFC) and brain response to verum EA in S1, SMA, and PFC were correlated with pain reduction following stimulation. Thus, while greater activation to verum acupuncture in these regions may predict subsequent analgesia, PFC activation may specifically mediate reduced pain when stimulating distal acupoints.
Figures

References
-
- Kiernan MC, Mogyoros I, Burke D. Conduction block in carpal tunnel syndrome. Brain. 1999;122(5):933–941. - PubMed
-
- Yang C, Hsieh C, Wang N, et al. Acupuncture in patients with carpal tunnel syndrome a randomized controlled trial. Clinical Journal of Pain. 2009;25(4):327–333. - PubMed
-
- Kumnerddee W, Kaewtong A. Efficacy of acupuncture versus night splinting for carpal tunnel syndrome: a randomized clinical trial. Journal of the Medical Association of Thailand. 2010;93(12):1463–1469. - PubMed
-
- Yao E, Gerritz PK, Henricson E, et al. Randomized controlled trial comparing acupuncture with placebo acupuncture for the treatment of carpal tunnel syndrome. PM and R. 2012;4(5):367–373. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
