

Association of serum uric acid with 2-hour postload glucose in Chinese with impaired fasting plasma glucose and/or HbA1c
- PMID: 23844086
- PMCID: PMC3700996
- DOI: 10.1371/journal.pone.0067759
Association of serum uric acid with 2-hour postload glucose in Chinese with impaired fasting plasma glucose and/or HbA1c
Abstract
Objective: To examine whether serum uric acid (SUA) is associated with 2-hour postload glucose (2-h PG) in Chinese with impaired fasting plasma glucose (IFG) and/or HbA1c (IA1C).
Research design and methods: Anthropometric and biochemical examinations, such as SUA concentration, were performed in 3763 individuals from all the villages in Baqiao County, China. A 75-g oral glucose tolerance test (OGTT) was conducted in 1197 Chinese with prediabetes as having IFG (110 ≤ fasting plasma glucose [FPG] <126 mg/dl and HbA1c <6.5%), IA1C (5.7% ≤ HbA1c <6.5% and FPG <126 mg/dl), or both.
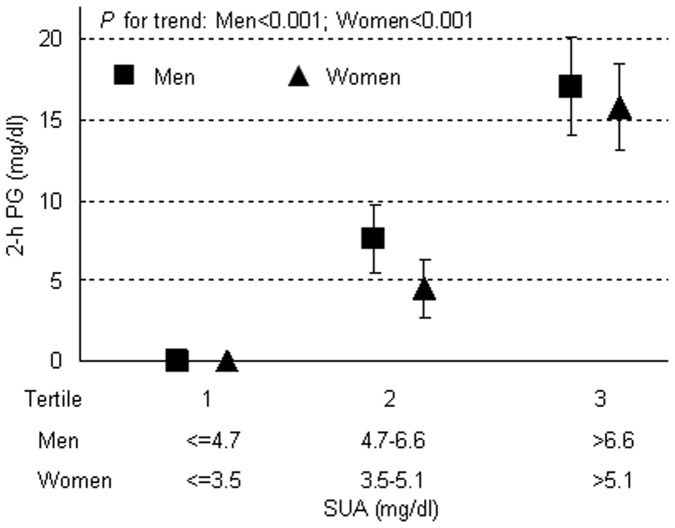
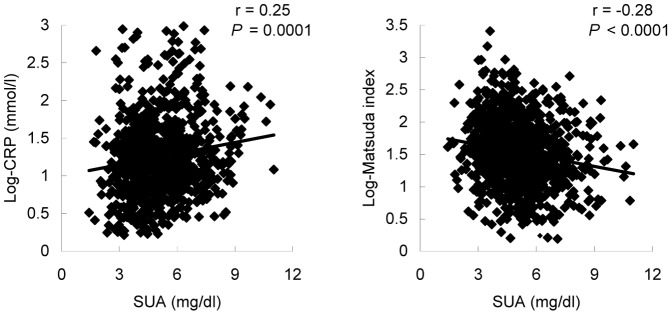
Results: The present study included 1197 participants with IFG and/or IA1C (mean age 56.5 ± 10.3 years; 50.6% men). In multivariate linear regression, after adjustment for gender, age, smoking and drinking, body mass index (BMI), systolic and diastolic blood pressure (SBP, DBP), lipid profiles, logarithmic transformed C-reactive protein (log-CRP), estimated glomerular filtration rate (e-GFR), FPG and HbA1c, with a 1-mg/dl increment of SUA, 2-h PG increased by 5.04 ± 0.72 (P<0.001), 3.06 ± 1.08 (P = 0.001), 5.40 ± 1.26 (P<0.001), and 2.34 ± 2.16 mg/dl (P = 0.056) in all participants, in participants with normal glucose tolerance (NGT), with impaired glucose tolerance (IGT), and with 2-h newly diagnosed diabetes (2-h NDM, with 2-h PG ≥ 200 mg/dl), respectively. In both men and women, 2-h PG increased progressively and significantly from the lower to the upper SUA tertiles (P<0.001). Moreover, in multivariate logistic regression, 1-standard deviation (SD; 1.53 mg/dl) increment of SUA was significantly associated with a 36% higher risk for 2-h NDM (Odds ratio [CI 95%]: 1.36 [1.09-1.99]; P = 0.03).
Conclusions: SUA is significantly associated with 2-h PG in Chinese with IFG and/or IA1C.
Conflict of interest statement
Figures
Similar articles
-
[Association of Serum Uric Acid with 2-hour Postload Glucose in Predibetic Patients].Sichuan Da Xue Xue Bao Yi Xue Ban. 2015 Sep;46(5):750-3. Sichuan Da Xue Xue Bao Yi Xue Ban. 2015. PMID: 26619550 Chinese.
-
Fluctuation between fasting and 2-H postload glucose state is associated with chronic kidney disease in previously diagnosed type 2 diabetes patients with HbA1c ≥ 7%.PLoS One. 2014 Jul 21;9(7):e102941. doi: 10.1371/journal.pone.0102941. eCollection 2014. PLoS One. 2014. PMID: 25047354 Free PMC article.
-
Serum uric acid is more strongly associated with impaired fasting glucose in women than in men from a community-dwelling population.PLoS One. 2013 Jun 13;8(6):e65886. doi: 10.1371/journal.pone.0065886. Print 2013. PLoS One. 2013. PMID: 23785457 Free PMC article.
-
Association of C-reactive protein levels with fasting and postload glucose levels according to glucose tolerance status.Arch Med Res. 2014 Jan;45(1):70-5. doi: 10.1016/j.arcmed.2013.11.004. Epub 2013 Dec 8. Arch Med Res. 2014. PMID: 24326321
-
The Oral Glucose Tolerance Test: 100 Years Later.Diabetes Metab Syndr Obes. 2020 Oct 19;13:3787-3805. doi: 10.2147/DMSO.S246062. eCollection 2020. Diabetes Metab Syndr Obes. 2020. PMID: 33116727 Free PMC article. Review.
Cited by
-
Serum Uric Acid Levels were Dynamically Coupled with Hemoglobin A1c in the Development of Type 2 Diabetes.Sci Rep. 2016 Jun 22;6:28549. doi: 10.1038/srep28549. Sci Rep. 2016. PMID: 27328642 Free PMC article.
-
Common variants related to serum uric acid concentrations are associated with glucose metabolism and insulin secretion in a Chinese population.PLoS One. 2015 Jan 24;10(1):e0116714. doi: 10.1371/journal.pone.0116714. eCollection 2015. PLoS One. 2015. PMID: 25617895 Free PMC article.
References
-
- Fang J, Alderman MH (2000) Serum uric acid and cardiovascular mortality the NHANES I epidermiologic follow-up study, 1971–1992. National Health and Nutrition Examination Survey. JAMA 283: 2404–2410. - PubMed
-
- Culleton B, Larson M, Kannel W, Levy D (1999) Serum uric acid and risk for cardiovascular diasease and death: the Framingham heart study. Ann Intern Med 131: 7–13. - PubMed
-
- Verdecchia P, Schillaci G, Reboldi G, Santeusanio F, Porcellati C, et al. (2000) Relation between serum uric acid and risk of cardiovascular disease in essential hypertension. The PIUMA study. Hypertension 36: 1072–1078. - PubMed
-
- Bos MJ, Koudstaal PJ, Hofman A, Witteman JC (2006) BretelerMM (2006) Uric acid is a risk factor for myocardial infarction and stroke: the Rotterdam study. Stroke 37: 1503–1507. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
