

Cortical hand bone porosity and its association with distal radius fracture in middle aged and elderly women
- PMID: 23844197
- PMCID: PMC3700909
- DOI: 10.1371/journal.pone.0068405
Cortical hand bone porosity and its association with distal radius fracture in middle aged and elderly women
Abstract
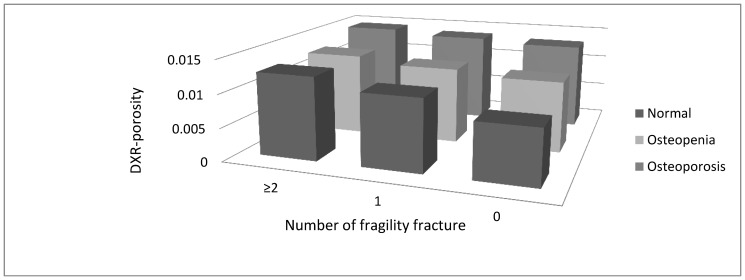
Objective: Reduced bone mineral density (BMD), assessed by Dual Energy X-ray absorptiometry (DXA), is a well-known risk factor for fragility fracture. A large proportion of patients with fracture have only slightly reduced BMD. Assessment of other bone structure features than BMD may improve identification of individuals at increased fracture risk. Digital X-ray radiogrammetry (DXR), which is a feasible tool for measurement of metacarpal cortical bone density, also gives an estimate of cortical bone porosity. Our primary aim was to explore the association between cortical porosity in the hand assessed by DXR and distal radius fracture.
Methods: This case-control study included 123 women >50 years with distal radius fracture, and 170 controls. DXR was used to measure metacarpal BMD (DXR-BMD), cortical porosity (DXR-porosity), thickness (DXR-CT) and bone width (DXR-W) of the hand. Femoral neck BMD was measured by DXA.
Results: The fracture group had a statistically significant lower DXR-BMD (0.492 vs. 0.524 g/cm(2) p<0.001), higher cortical DXR-porosity (0.01256 vs. 0.01093, p<0.001), less DXR-CT (0.148 vs. 0.161 cm, p<0.001) and lower femoral neck DXA-BMD (0.789 vs. 0.844 g/cm(2), p = 0.001) than the controls. In logistic regression analysis adjusted for age, a significant association with distal radius fracture (OR, 95% CI) was found for body mass index (0.930, 0.880-0.983), DXA-BMD (0.996, 0.995-0.999), DXR-BMD (0.990, 0.985-0.998), DXR-porosity (1.468, 1.278-1.687) and DXR-CT (0.997, 0.996-0.999). In an adjusted model, DXR-porosity remained the only variable associated with distal radius fracture (1.415, 1.194-1.677).
Conclusion: DXR derived porosity is associated with fracture at distal radius and might be a sensitive marker for skeletal fragility.
Conflict of interest statement
Figures
References
-
- Holroyd C, Cooper C, Dennison E (2008) Epidemiology of osteoporosis. BestPractResClinEndocrinolMetab 22: 671–685. - PubMed
-
- Oyen J, Rohde GE, Hochberg M, Johnsen V, Haugeberg G (2010) Low-energy distal radius fractures in middle-aged and elderly women-seasonal variations, prevalence of osteoporosis, and associates with fractures. OsteoporosInt 21: 1247–1255. - PubMed
-
- Siris ES, Chen YT, Abbott TA, Barrett-Connor E, Miller PD, et al. (2004) Bone mineral density thresholds for pharmacological intervention to prevent fractures. ArchInternMed 164(10): 1108–1112. - PubMed
-
- Oyen J, Brudvik C, Gjesdal CG, Tell GS, Lie SA, et al. (2011) Osteoporosis as a risk factor for distal radial fractures: a case-control study. JBone Joint SurgAm 93: 348–356. - PubMed
-
- Bouxsein ML, Karasik D (2006) Bone geometry and skeletal fragility. CurrOsteoporosRep 4(2): 49–56. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
