

Direct-acting antivirals for the treatment of chronic hepatitis C: open issues and future perspectives
- PMID: 23844410
- PMCID: PMC3687480
- DOI: 10.1155/2013/704912
Direct-acting antivirals for the treatment of chronic hepatitis C: open issues and future perspectives
Abstract
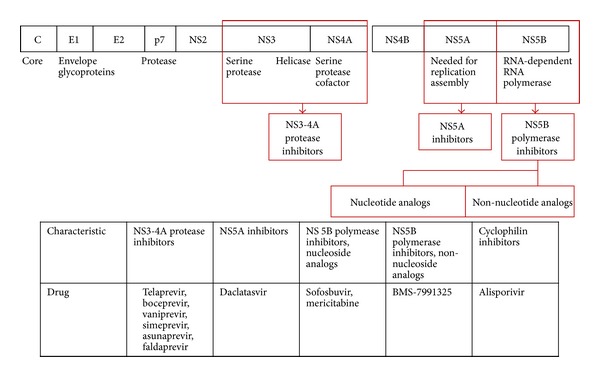
Currently, two direct-acting antivirals (DAAs) show well-established efficacy against hepatitis C virus (HCV), namely, first-wave protease inhibitors telaprevir and boceprevir. Most clinical trials have examined DAAs in combination with standard of care (SOC) regimens. Future therapeutic drugs were divided into three categories. They are second-wave protease inhibitors, second-generation protease inhibitors, and polymerase inhibitors. Second-wave protease inhibitors are more improved form and can be administered once a day. Oral drug combinations can be favored because interferon (IFN) not only has to be given as intradermal injection, but also can cause several serious side effects. Combination of drugs with different mechanisms shows a good sustained virological response (SVR). But several mutations are associated with viral resistance to DAAs. Therefore, genotypic resistance data may provide insights into strategies aimed at maximizing SVR rates and minimizing resistance. Combined drug regimens are necessary to prevent the emergence of drug-resistant HCV. Many promising DAA candidates have been identified. Of these, a triple regimen containing sofosbuvir shows promise, and treatment with daclatasvir plus asunaprevir yields a high SVR rate (95%). Oral drug combinations will be standard of care in the near future.
Figures

References
-
- Stedman CA. Current prospects for interferon-free treatment of hepatitis C in 2012. Journal of Gastroenterology and Hepatology. 2013;28:38–45. - PubMed
-
- McGovern B, Abu Dayyeh B, Chung RT. Avoiding therapeutic pitfalls: the rational use of specifically targeted agents against hepatitis C infection. Hepatology. 2008;48:1700–1712. - PubMed
-
- U.S Food and Drug Administration. FDA news release. FDA approves Incivek for hepatitis C, May 2011, http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm256299.htm.
-
- U.S Food and Drug Administration. FDA news release. FDA approves Incivek for hepatitis C, May 2011, http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm255390.htm.
-
- Vectrelis (boceprevir) capsules. Merck. May 2011, http://www.accessdata.fda.gov/drugsatfda_docs/label/2011/202258lbl.pdf.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
