

A core microbiome associated with the peritoneal tumors of pseudomyxoma peritonei
- PMID: 23844722
- PMCID: PMC3729368
- DOI: 10.1186/1750-1172-8-105
A core microbiome associated with the peritoneal tumors of pseudomyxoma peritonei
Abstract
Background: Pseudomyxoma peritonei (PMP) is a malignancy characterized by dissemination of mucus-secreting cells throughout the peritoneum. This disease is associated with significant morbidity and mortality and despite effective treatment options for early-stage disease, patients with PMP often relapse. Thus, there is a need for additional treatment options to reduce relapse rate and increase long-term survival. A previous study identified the presence of both typed and non-culturable bacteria associated with PMP tissue and determined that increased bacterial density was associated with more severe disease. These findings highlighted the possible role for bacteria in PMP disease.
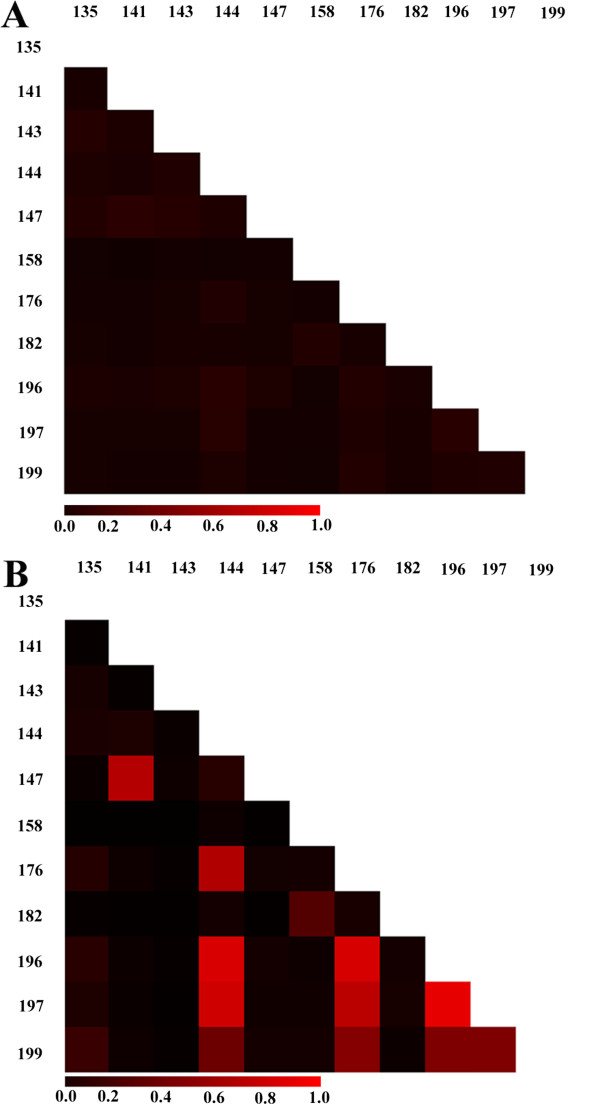
Methods: To more clearly define the bacterial communities associated with PMP disease, we employed a sequenced-based analysis to profile the bacterial populations found in PMP tumor and mucin tissue in 11 patients. Sequencing data were confirmed by in situ hybridization at multiple taxonomic depths and by culturing. A pilot clinical study was initiated to determine whether the addition of antibiotic therapy affected PMP patient outcome.
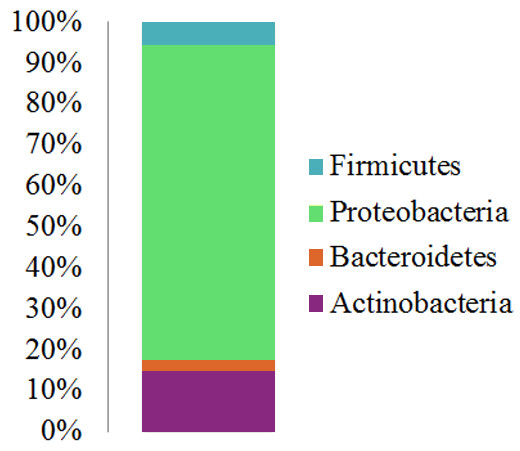
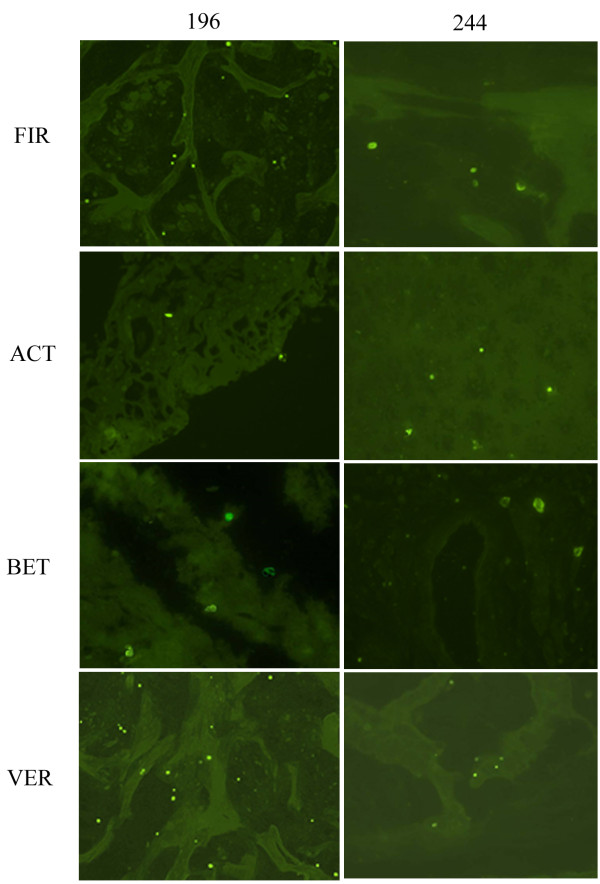
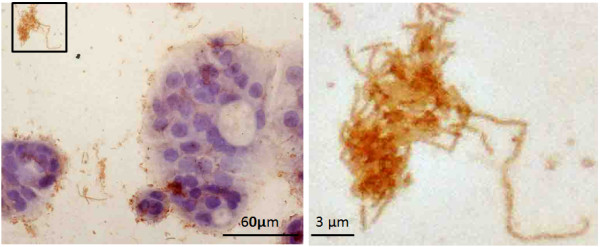
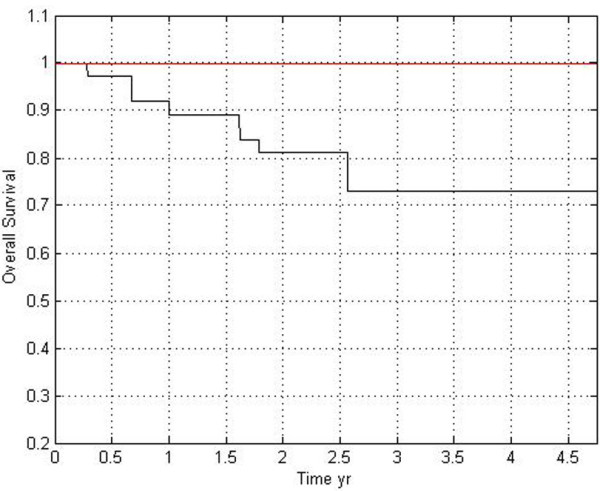
Main results: We determined that the types of bacteria present are highly conserved in all PMP patients; the dominant phyla are the Proteobacteria, Actinobacteria, Firmicutes and Bacteroidetes. A core set of taxon-specific sequences were found in all 11 patients; many of these sequences were classified into taxonomic groups that also contain known human pathogens. In situ hybridization directly confirmed the presence of bacteria in PMP at multiple taxonomic depths and supported our sequence-based analysis. Furthermore, culturing of PMP tissue samples allowed us to isolate 11 different bacterial strains from eight independent patients, and in vitro analysis of subset of these isolates suggests that at least some of these strains may interact with the PMP-associated mucin MUC2. Finally, we provide evidence suggesting that targeting these bacteria with antibiotic treatment may increase the survival of PMP patients.
Conclusions: Using 16S amplicon-based sequencing, direct in situ hybridization analysis and culturing methods, we have identified numerous bacterial taxa that are consistently present in all PMP patients tested. Combined with data from a pilot clinical study, these data support the hypothesis that adding antimicrobials to the standard PMP treatment could improve PMP patient survival.
Figures

Similar articles
-
Secreted mucins in pseudomyxoma peritonei: pathophysiological significance and potential therapeutic prospects.Orphanet J Rare Dis. 2014 May 5;9:71. doi: 10.1186/1750-1172-9-71. Orphanet J Rare Dis. 2014. PMID: 24886459 Free PMC article. Review.
-
Pseudomyxoma peritonei: is disease progression related to microbial agents? A study of bacteria, MUC2 AND MUC5AC expression in disseminated peritoneal adenomucinosis and peritoneal mucinous carcinomatosis.Ann Surg Oncol. 2008 May;15(5):1414-23. doi: 10.1245/s10434-007-9778-9. Epub 2008 Feb 26. Ann Surg Oncol. 2008. PMID: 18299935 Free PMC article.
-
Cross-laboratory replication of pseudomyxoma peritonei tumor microbiome reveals reproducible microbial signatures.mSphere. 2025 Mar 25;10(3):e0065224. doi: 10.1128/msphere.00652-24. Epub 2025 Feb 20. mSphere. 2025. PMID: 39976448 Free PMC article.
-
Antibiotic treatment decreases microbial burden associated with pseudomyxoma peritonei and affects β-catenin distribution.Clin Cancer Res. 2013 Jul 15;19(14):3966-76. doi: 10.1158/1078-0432.CCR-13-0616. Epub 2013 Jun 6. Clin Cancer Res. 2013. PMID: 23743566 Clinical Trial.
-
The etiology, clinical presentation, and management of pseudomyxoma peritonei.Surg Oncol Clin N Am. 2003 Jul;12(3):585-603. doi: 10.1016/s1055-3207(03)00026-7. Surg Oncol Clin N Am. 2003. PMID: 14567019 Review.
Cited by
-
Under the Hood: Understanding the Features of Mucin in Pseudomyxoma Peritonei.J Clin Med. 2023 Jun 12;12(12):4007. doi: 10.3390/jcm12124007. J Clin Med. 2023. PMID: 37373701 Free PMC article.
-
Secreted mucins in pseudomyxoma peritonei: pathophysiological significance and potential therapeutic prospects.Orphanet J Rare Dis. 2014 May 5;9:71. doi: 10.1186/1750-1172-9-71. Orphanet J Rare Dis. 2014. PMID: 24886459 Free PMC article. Review.
-
Fusobacterium nucleatum Is Associated with Tumor Characteristics, Immune Microenvironment, and Survival in Appendiceal Cancer.Microorganisms. 2025 Jul 11;13(7):1644. doi: 10.3390/microorganisms13071644. Microorganisms. 2025. PMID: 40732152 Free PMC article.
-
Fulfilling the Promise of Microbiomics to Revolutionize Medicine.J Microbiol Exp. 2015;2(3):00050. doi: 10.15406/jmen.2015.02.00050. Epub 2015 Aug 11. J Microbiol Exp. 2015. PMID: 27030825 Free PMC article. No abstract available.
-
Progress in Biological Research and Treatment of Pseudomyxoma Peritonei.Cancers (Basel). 2024 Apr 3;16(7):1406. doi: 10.3390/cancers16071406. Cancers (Basel). 2024. PMID: 38611084 Free PMC article. Review.
References
-
- Ronnett BM, Zahn CM, Kurman RJ, Kass ME, Sugarbaker PH, Shmookler BM. Disseminated peritoneal adenomucinosis and peritoneal mucinous carcinomatosis. A clinicopathologic analysis of 109 cases with emphasis on distinguishing pathologic features, site of origin, prognosis, and relationship to “pseudomyxoma peritonei”. Am J Surg Pathol. 1995;19:1390–1408. doi: 10.1097/00000478-199512000-00006. - DOI - PubMed
-
- Loungnarath R, Causeret S, Bossard N, Faheez M, Sayag-Beaujard AC, Brigand C, Gilly F, Glehen O. Cytoreductive surgery with intraperitoneal chemohyperthermia for the treatment of pseudomyxoma peritonei: a prospective study. Dis Colon Rectum. 2005;48:1372–1379. doi: 10.1007/s10350-005-0045-5. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
