

Renal survival in proteinase 3 and myeloperoxidase ANCA-associated systemic vasculitis
- PMID: 23846462
- PMCID: PMC3789333
- DOI: 10.2215/CJN.01020113
Renal survival in proteinase 3 and myeloperoxidase ANCA-associated systemic vasculitis
Abstract
Background and objectives: This study evaluated predictors for patient and renal survival in patients with ANCA-associated vasculitis (AAV) with and without renal involvement.
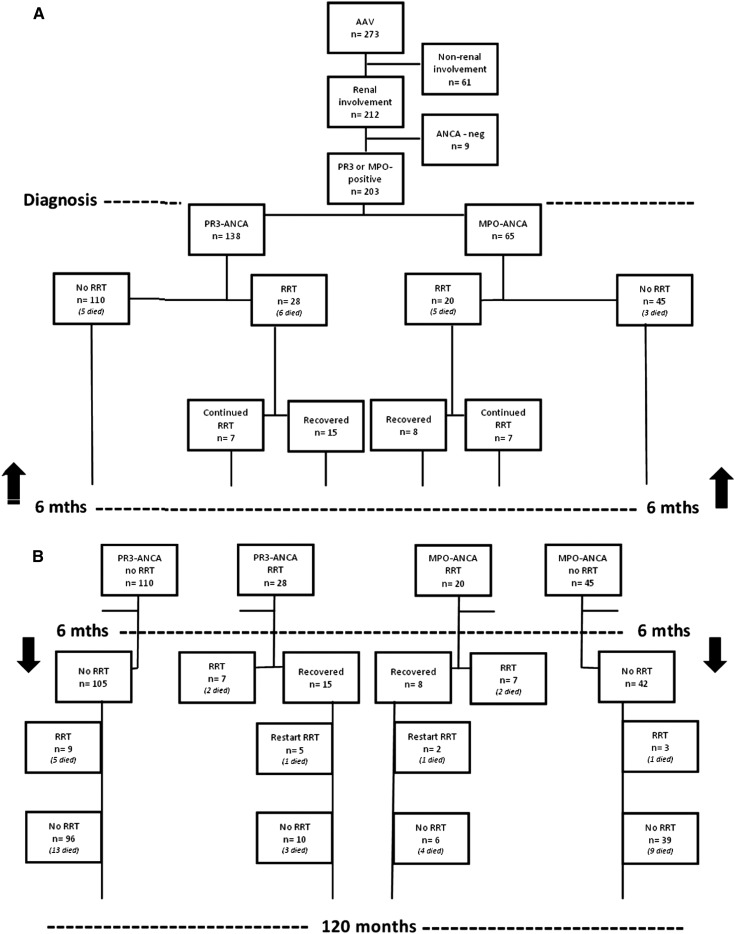
Design, setting, participants, & measurements: There were 273 consecutive AAV patients from January 1990 until December 2007 who were followed until death, loss to follow-up, or December 2010. Based on organ involvement, patients were divided into renal (n=212) and nonrenal groups (n=61). The primary end point was ESRD requiring renal replacement therapy (RRT) or renal transplantation or death.
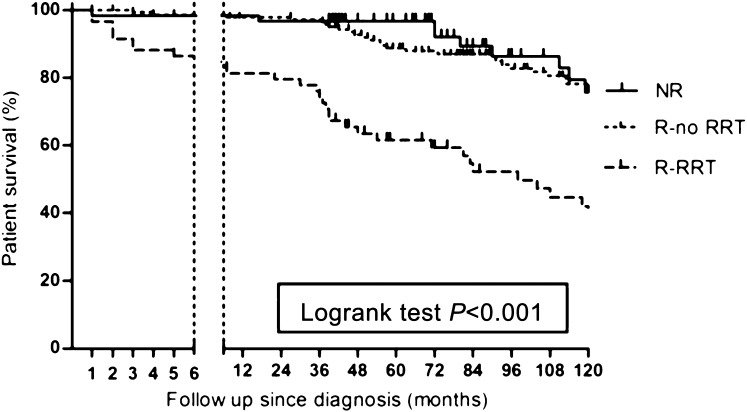
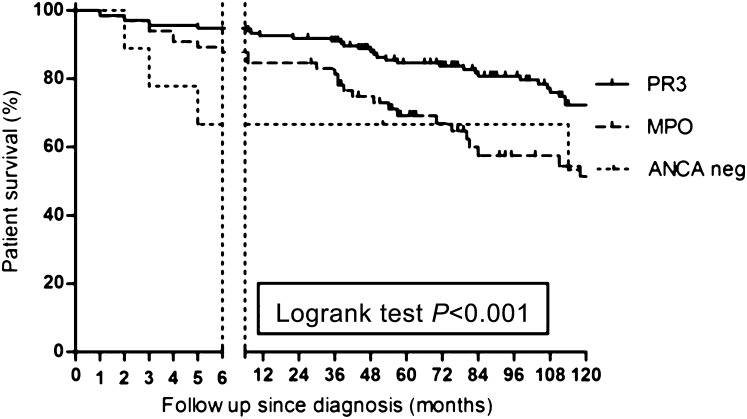
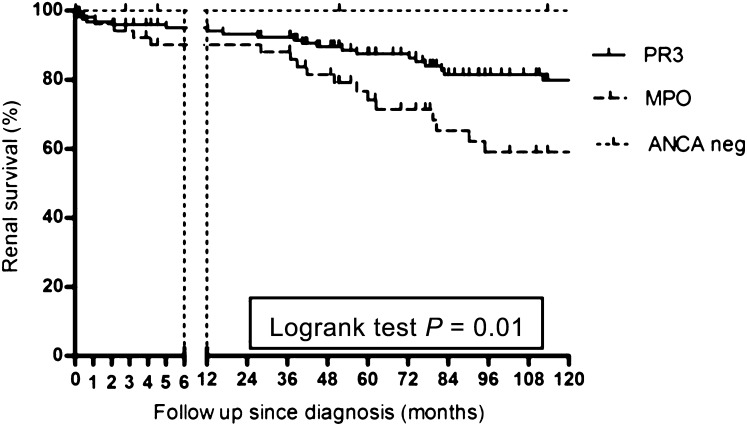
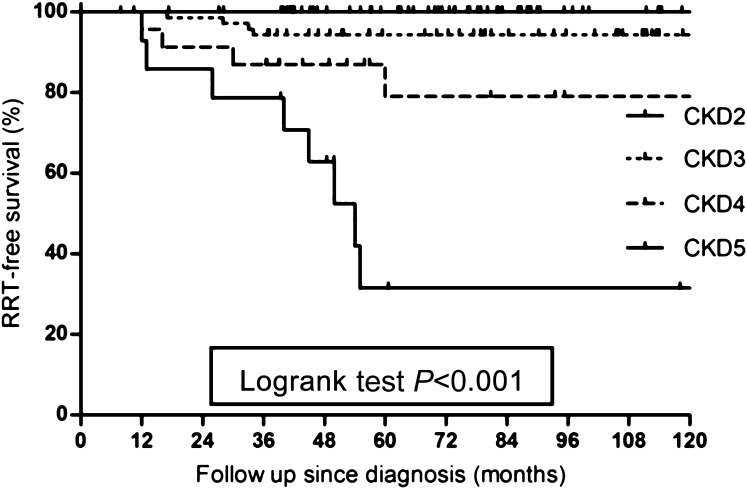
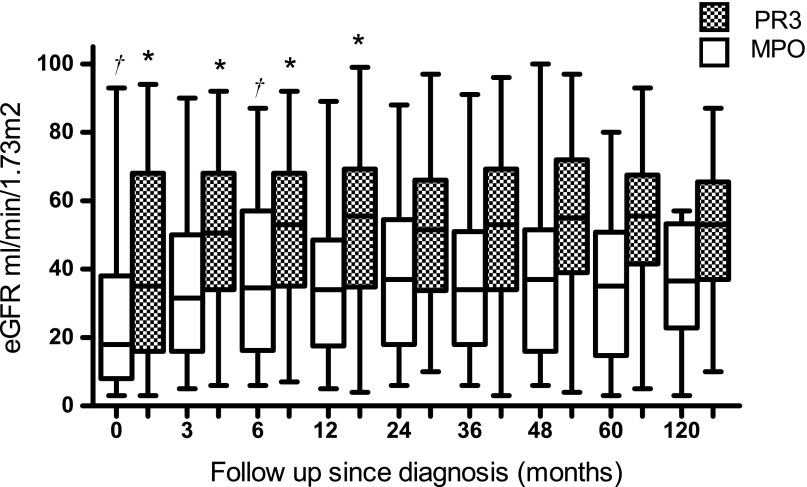
Results: Patient survival was significantly better in the nonrenal group compared with the renal group (hazard ratio, 0.55; 95% confidence interval, 0.33 to 0.92; P=0.02). In the renal group, renal survival was significantly worse in MPO-ANCA-positive patients (n=65) compared with PR3-ANCA-positive patients (n=138) (hazard ratio, 2.1; 95% confidence interval, 1.11 to 3.8; P=0.01). Of 48 patients who needed RRT at diagnosis, 11 patients (23%) died within 6 months and 14 patients (29%) did not regain renal function. Of all 23 patients who regained renal function after RRT, 7 patients (30%) were temporarily dialysis independent and needed dialysis later (range, 13-63 months). Five patients had a renal relapse in the 6 months before restart of RRT. Of all 203 PR3-ANCA-positive and MPO-ANCA-positive patients with renal involvement, 12 patients (6%) developed ESRD during follow-up. These patients were classified as CKD stage 4 or 5 after initial treatment and eight patients had a renal relapse before becoming dialysis dependent.
Conclusions: AAV patients with renal involvement who needed RRT had the worst survival probability. In multivariate analysis, the only major determinants for long-term renal survival were renal function at 6 months and renal relapses.
Figures
References
-
- Falk RJF, Jennette JC: ANCA small-vessel vasculitis. J Am Soc Nephrol 8: 314–322, 1997 - PubMed
-
- Franssen CFM, Stegeman CA, Kallenberg CGM, Gans ROB, De Jong PE, Hoorntje SJ, Tervaert JW: Antiproteinase 3- and antimyeloperoxidase-associated vasculitis. Kidney Int 57: 2195–2206, 2000 - PubMed
-
- Slot MC, Tervaert JW, Franssen CFM, Stegeman CA: Renal survival and prognostic factors in patients with PR3-ANCA associated vasculitis with renal involvement. Kidney Int 63: 670–677, 2003 - PubMed
-
- Westman KWA, Bygren PG, Olsson H, Ranstam J, Wieslander J: Relapse rate, renal survival, and cancer morbidity in patients with Wegener’s granulomatosis or microscopic polyangiitis with renal involvement. J Am Soc Nephrol 9: 842–852, 1998 - PubMed
-
- Booth AD, Almond MKA, Burns A, Ellis P, Gaskin G, Neild GH, Plaisance M, Pusey CD, Jayne DR, Pan-Thames Renal Research Group : Outcome of ANCA-associated renal vasculitis: A 5-year retrospective study. Am J Kidney Dis 41: 776–784, 2003 - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
